
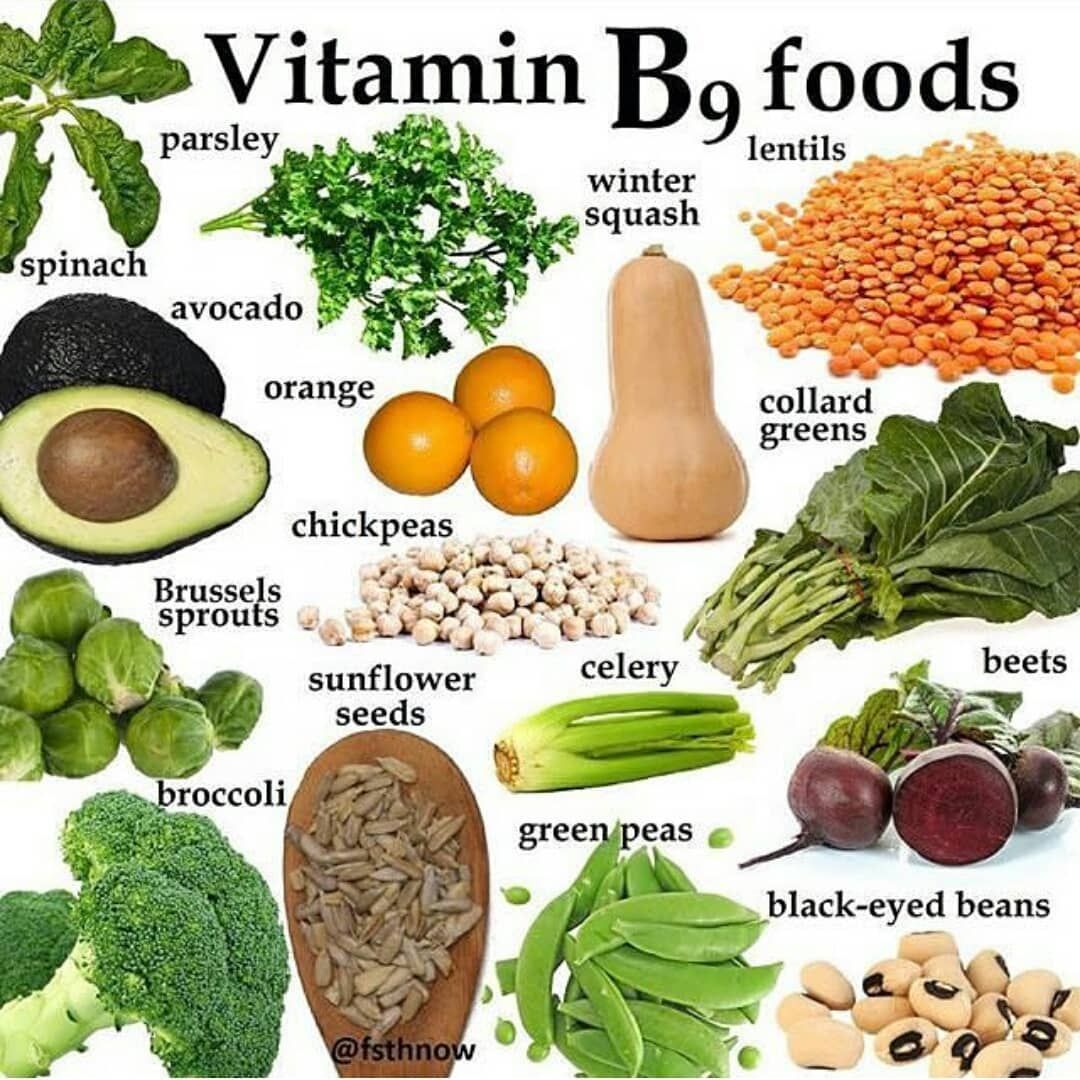
B9, also known as folate, is a water-soluble micronutrient central to health and homeostasis (Sanvisens et al., 2017). Functions include the metabolism of nutrients such as choline, amino acids, pyrimidines, purines, DNA synthesis/repair, and cell division (Gropper, Smith, & Carr, 2018). As such, deficiencies in folate can lead to disruptions in said functions. As a means of detecting and solving folate deficiency, the following will consider in greater detail, functions of folate, markers of deficiency, and its relationship to homocysteine.
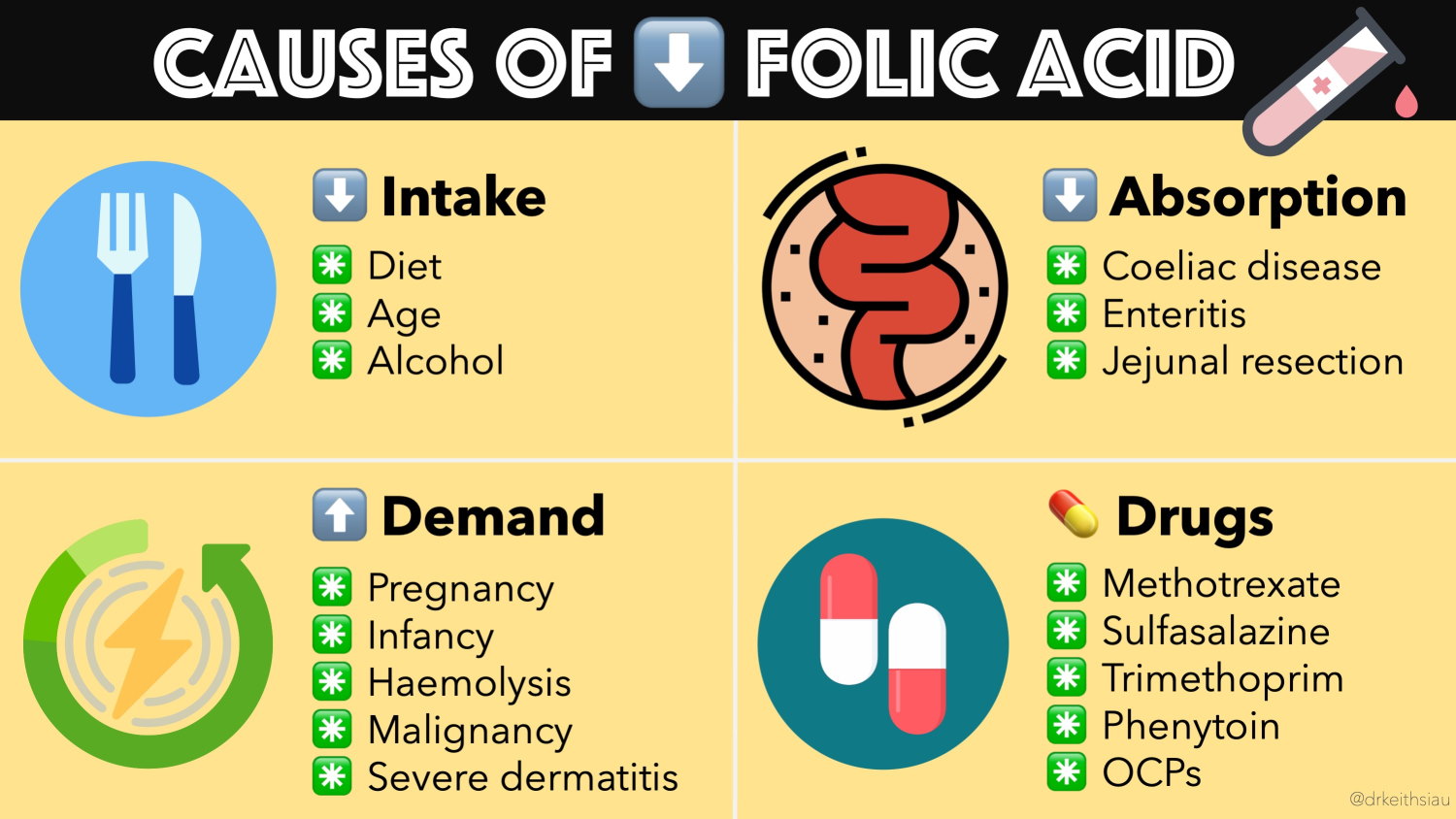
B9 deficiency can find its genesis from multiple sources to include impaired liver uptake, malabsorptive conditions, reduced storage, some drugs, and excessive renal excretion (Sanvisens et al., 2017). Such physiological aberrations can manifest into conditions such as cognitive impairment and megaloblastic anemia (abnormal red blood cells). Furthermore, B9 deficiency has also been associated with an increased risk of colorectal/breast cancer, malignancy, and the progression of alcohol-related liver disease (Sanvisens et al., 2017). Having considered the conditions associated with B9 deficiency, the following will explore methods in tracking B9 status and its relationship to homocysteine.
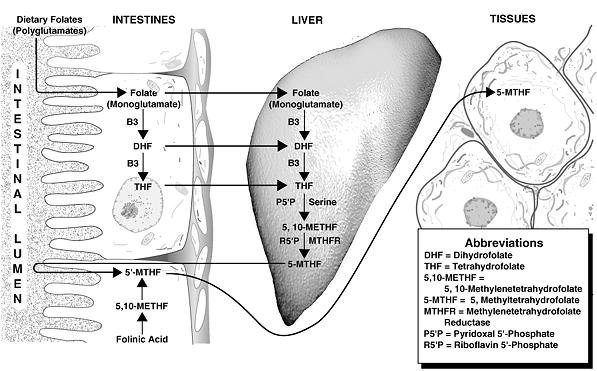
Folic acid (the oxidized and supplemental form of folate) is absorbed in the small bowl once it has been hydrolyzed (chemical breakdown with the use of water) into monoglutamate from polyglutamate (Gropper at al., 2018; Sanvisens et al., 2017). Such a vitamin is central to cellular growth and division of leukocytes, erythrocytes, and platelets (Sanvisens et al., 2017). Furthermore, B9 maintains metabolic processes such as the synthesis of nucleic acids and homocysteine methylation (Sanvisens et al., 2017). Serum folate measures recent digestion of B9 and therefore is not truly representative of long-term/stored B9. As such, serum folate is not an adequate biomarker to track potential deficiency unless multiple measures are taken (Sanvisens et al., 2017).
Tracking folate through erythrocyte stores is a better reflection of long-term levels of said micronutrient. Furthermore, such a measurement will reflect body stores within weeks of insufficient ingestion, allowing the opportunity for intervention before signs and symptoms worsen. Gropper et al. (2018) stated that red blood cell concentrations less than 140 ng/ml suggesting deficiency.
If plasma/serum measures are procured, Sanvisens et al. (2018) stated that the reference range would be between 2-20 ng/ml, while Gropper et al. (2018) indicated that levels below 3 ng/ml indicated deficiency. If folate levels are determined to be deficient, supplementation with 1-5 mg of folate daily until red blood cell/plasma/serum levels begin to fall within respective ranges (Grooper et al., 2018). Having reviewed B9 deficiency, symptoms, methods of measurement, and reference ranges, the following will consider factors behind inadequate folate metabolism and its relationship to homocysteine.
Lower folate levels can emanate from multiple sources to include genetic and environmental (i.e., alcohol consumption, obesity, smoking) factors (Vidmar, Grzelj, Mlinaric-Rascan, Gersak, & Sollner-Dolenc, 2018). Metabolism of folate requires the implementation of enzymes, such as methylenetetrahydrofolate reductase (MTHFR), which are expressed through the MTHFR gene.
However, if said genes are formed incorrectly (i.e., polymorphism) such enzymes necessary for folate metabolism and transport can become compromised (Vidmar et al., 2018). Inadequate B9 metabolism also affects homocysteine levels; a toxic metabolite that is neutralized in a well-functioning body (Vidmar et al., 2018).
Furthermore, elevated homocysteine levels are associated with hyperlipidemia, hypertension, retinal vein occlusion, and venous thromboembolism (Vidmar et al., 2018). Conversely, supplemental folate has been shown to reverse the same, helping establish the relationship between B9 and homocysteine (Vidmar et al., 2018).
In conclusion, B9 is a water-soluble micronutrient central to homeostasis and is involved in the metabolism of nutrients such as choline, amino acids, pyrimidines, purines, DNA synthesis/repair, and cell division. As such, maintaining adequate folate levels is another key in sustaining health and longevity.
References
Gropper, S. S., Smith, J. L., & Carr, T. P. (2018). Advanced nutrition and human metabolism (7thed.). Boston, MA: Cengage Learning.
Sanvisens, A., Zuluaga, P., Pineda, M., Fuster, D., Bolao, F., Junca, J., Tor, J., … Muga, R. (2017). Folate deficiency in patients seeking treatment of alcohol use disorder. Drug and Alcohol Dependence, 180, 417-422.
Vidmar, M., Grzelj, J., Mlinaric-Rascan, I., Gersak, K., & Sollner-Dolenc, M. (2018). Medicines associated with folate-homocysteine-methionine pathway disruption. Archives of Toxicology, 1-25.
-Michael McIsaac