
Hypertension (HT) is a condition and form of cardiovascular disease (CVD) which has generally manifested in adults. However, HT currently affects an approximated 3-5% of children and up to 10-11% of adolescent populations, worldwide.1 Furthermore, HT has been estimated to affect 1 in 3 Americans, or approximately 76,400,000 individuals and has accounted for as many as 36,000 deaths in 2009.2
HT’s genesis is multifactorial and is associated with other pathophysiological conditions which may cause, or worsen, abnormally high blood pressure.1(3) As such, it is imperative to develop thoroughly constructed interventions aimed at preventing and/or mitigating HT. In addition to introducing physical activity, a commonly understood tool to maintain cardiovascular health, it is equally imperative to consider nutritional interventions to support the same. Thus, in the following sections, botanicals will be considered as well as their effects upon HT.
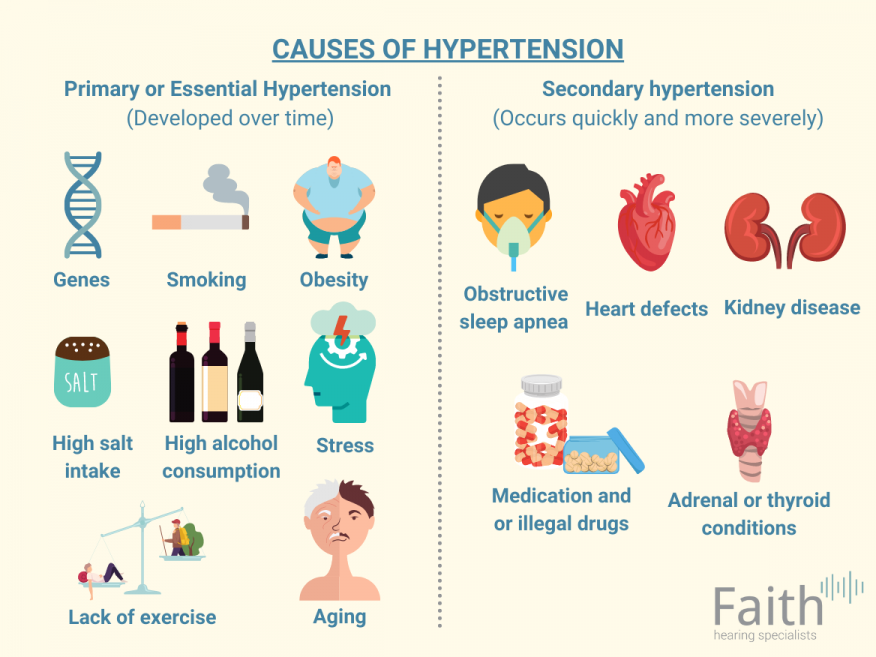
As mentioned in the introduction, individuals with HT often exhibit other pathophysiological conditions to include exaggerated immune system activation, accelerated arterial aging, sympathetic nervous system activation, oxidative stress, metabolic syndrome (i.e., hyperinsulinemia), accelerated biological maturation, visceral obesity, and decreased ratio of lean mass.1(3) It is likely then, that the presence of such conditions are contributing to, and worsening, HT.
Although pharmaceutical medications can lower blood pressure, an emerging interest from the public to find alternative therapies with less side effects have been taking place.2(10) Biesinger et al2(10) indicated that several studies have explored the effectiveness of botanically derived phytochemicals in managing high blood pressure, defined as 130/85 (systolic/diastolic). However, said studies might have had limitations as they considered the efficacy of individual polyphenolic agents upon HT. Such research did not explore the potential synergistic effects of botanicals when consumed as an aggregate; a point of interest for Biesinger et al2(10)
![]()
As a means of exploring the potential therapeutic efficacy behind the concurrent use of multiple botanicals in managing HT, Biesinger et al2(10) constructed a study exploring the same. Dosages for said botanicals were as follows: grape seed (330 mg), green tea (100 mg), resveratrol (60 mg), quercetin/ginkgo biloba/bilberry (60 mg).2(10) Participants were screened and accepted into the study if they met 3 out of the 5 criteria for metabolic syndrome: blood pressure (mm Hg) ⩾130 systolic or ⩾ 85 diastolic, fasting glucose ⩾ 5.55, waist circumference ⩾ 102 men or ⩾ 88 women, triglyceride levels (mmol/l), ⩾ 1.69, HDL (mmol/l) ⩽ 1.03 men or ⩽ 1.29 women.2(11)
Exclusion criteria included alcohol consumption in excess of 12 drinks weekly, BMI over 40 kg/m2, history of prior cardiovascular event liver disease, diabetes, use of calcium/magnesium antacids, renal insufficiency, chronic disease that might interfere with participation, and an unwillingness to stop current dietary supplement intake.2(11)

Of the 29 volunteers who were recruited for said study, 18 participants met the eligibility criteria and finished the protocol.2(11) Participants were assigned via random draw to a 28-day supplement or a 28-day placebo group, while subjects and researchers were blinded to the true nature of bottles containing either the placebo or combined botanicals.2(12) In addition to inclusion criteria at baseline, other baseline measures included total cholesterol, low-density lipoprotein cholesterol (LDL-C), body mass index, serum cytokines, and mean arterial pressure.2(11)
After the study was completed, particular findings emerged to include a reduction in blood pressure, specifically diastolic blood pressure, amongst participants in the intervention group.2(13) Furthermore, a trend toward reduction in mean arterial pressure was also found from participants who used combined botanicals throughout the study, and such changes were thought to derive from the increased presence of nitric oxide (a vasodilator) found in the experimental group.2(13,15)Finally, said changes occurred in the absence of weight loss, BMI reductions, or changes in daily nutrient intake suggesting said blood pressure changes were due solely from combined botanical use.2(13)
In conclusion, HT is a condition and form of CVD that impacts the adult population, 3-5% of children, and up to 10-11% of adolescent populations, worldwide. HT’s genesis is multifactorial and is associated with other pathophysiological conditions which may cause, or worsen, abnormally high blood pressure. Although physical activity is a commonly understood means of controlling blood pressure, botanicals have gained public attention as an alternative intervention to pharmaceutical drugs. Although the results of Biesinger et al2(15) are promising, the sample size was small due to drop outs which likely underpowered said findings. Despite said limitations, no side effects were noted from the combined botanicals, which suggests that implementation of the same would, at minimum, be safe and likely effective in helping manage HT.
References
1. Litwin M, Kulaga Z. Obesity, metabolic syndrome, and primary hypertension. Pediatr Nephrol. 2020:1-13. doi:https://doi.org/10.1007/s00467-020-04579-3.
2. Biesinger S, Michaels HA, Quadros AS, et al. A combination of isolated chemicals and botanical extracts lowers diastolic blood pressure in a randomized controlled trial of hypertensive subjects. Eur J Clin Nutr. 2016;70(1):10-16. doi:10.1038/ejcn.2015.88.
-Michael McIsaac