

Insulin resistance and type 2 diabetes are characterized by an impaired ability to metabolize glucose (Paoli, Rubini, Volek, & Grimaldi, 2013). However, the severity of insulin resistance and type 2 diabetes has been mitigated and/or eradicated by very low carbohydrate diets (Paoli et al., 2013). Considering the potential side effects of drug therapy interventions, nutritional protocols as a first line of defense would appear to be the most logical, least dangerous, and equally or more effective intervention to choose (Feinman et al., 2015). In the following sections, I would like to provide evidence that supports the aforementioned supposition, as a means to more deeply understand and appreciate the influence of nutrition in disease management.

Initially, it may be prudent to review the different permutations of carbohydrate-restricted protocols as a means of avoiding confusion and misinterpretation: the very low carbohydrate ketogenic diet is defined as 20-50 grams of carbohydrates per day with, or without, the presence of ketosis. The low carbohydrate diet is defined as less than 130 grams of carbohydrates per day. The moderate carbohydrate diet is defined as 26-45% of total daily caloric intake. Finally, the high carbohydrate diet is defined as approximately 49% of total daily caloric intake (Feinman et al., 2015). The following sections will provide points of evidence to help support the efficacy, and implementation, of low carbohydrate diets.
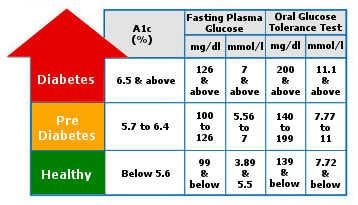
The first point of evidence that Feinman et al. (2015) offered suggested that carbohydrate restriction had the greatest effect of lowering blood glucose concentrations. Indeed, the first sign of an aberration in glucose metabolism is blood glucose levels between 7.8-11.O mmol/L approximately two hours after consuming a meal (Giugliano, Ceriello, Razzoli, & Esposito, 2008). Thus, controlling blood glucose levels is of the highest importance to avoid insulin resistance or overt diabetes. If dietary carbohydrates are universally understood, which they are, as a determinant of blood glucose concentrations, then a reduction of dietary carbohydrates could achieve this end, circumventing the use of endogenous or exogenous insulin (Feinman et al., 2015).
The second point of evidence indicated that during the growth period (1974-2000) of obesity and diabetes, excess caloric consumption was almost entirely due to increased carbohydrate consumption (Feinman et al., 2015). Feinman et al. (2015) substantiated this epidemiological measurement by biochemical mechanisms. That is, chronic and overstimulation of insulin from excess carbohydrate consumption causes a metabolic state in which fatty acids are stored (i.e., lipogenesis) as opposed to being broken down and used (i.e. lipolysis).
The aforementioned process causes an accumulation of fat within the liver, disrupting normal levels of very-low-density lipoproteins circulating in the bloodstream and the pancreas. This cycle, over time, impairs beta cell function within the pancreas, leading to impaired insulin function and glucose metabolism. Eventually, this cycle can lead to insulin resistance, and eventually, diabetes (Feinman et al., 2015).
![]()
The third and fourth points of evidence by Feinman et al. (2015) noted that carbohydrate restriction can improve hyperglycaemia without losing bodyweight. This is particularly important considering that not all individuals with diabetes are overweight, making the commonly held notion that caloric restriction and weight reduction alone improves hyperglycaemia.
This also provides opportunities for individuals who are overweight to experience results in improved blood glucose concentrations much sooner, instead of waiting to lose weight (Feinman et al., 2015). Comparisons of macronutrient manipulations (i.e., low fat/high carbohydrate vs. high fat/low carbohydrate) revealed compelling results; lower carbohydrate consumption outperformed higher carbohydrate consumption diet plans when total caloric consumption was maintained, both in terms of weight loss and improved blood glucose measures (Feinman et al., 2015).
The fifth point of evidence from Feinman et al. (2015) indicated that adherence to a low carbohydrate diet was as good, or better, than other dietary interventions (i.e., low fat/high carbohydrate) that were calorically identical. Such a finding helps support the implementation of a low carbohydrate intervention, and reassures individuals hesitant to initiate the protocol.
Another pertinent and appealing report from experimental subjects (from a low carbohydrate forum including over 150,000 members) included a suppressed appetite, and a strong sense of satiety when implementing the low carbohydrate intervention; a phenomenon not as prevalent when participating in low fat diets (Feinman et al., 2015). The authors posited that appetite suppression was engaged by modulating insulin-mediated signalling pathways that induces hunger in the brain (Feinman et al., 2015).

The sixth point of evidence suggested that low carbohydrate diets with moderate levels of protein had other beneficial outcomes when compared to low fat diets; subjects on low carbohydrate/higher protein diets lost less muscle mass than subjects on low fat dietary interventions (Feinman et al., 2015). Furthermore, low carbohydrate/higher protein diets produced higher resting metabolic rates and decreased markers (i.e., improved resting blood pressure and blood lipid profiles) of cardiovascular disease (Feinman et al., 2015).
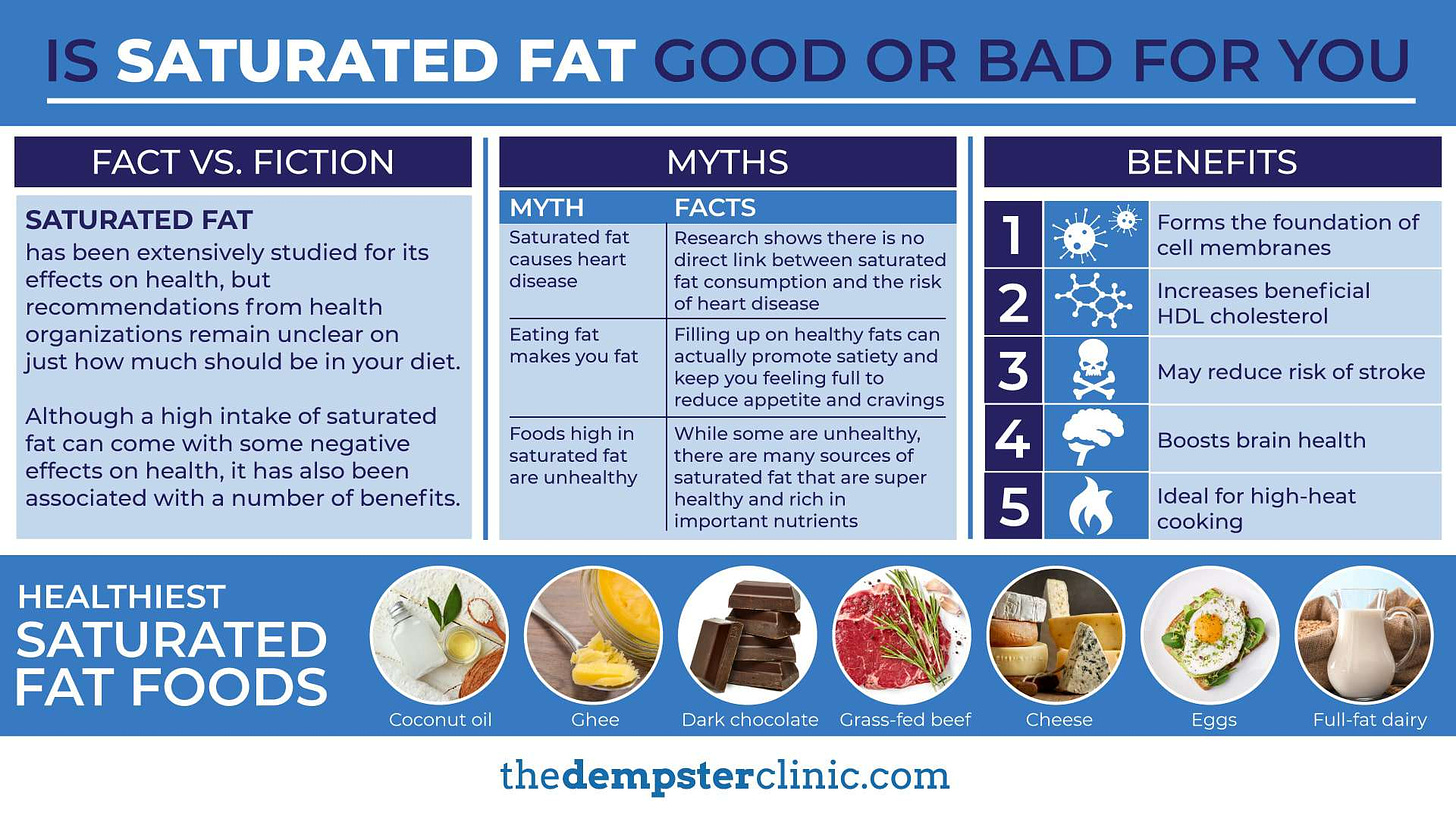
The seventh and eighth points of evidence dispelled the myth that saturated fats from low carbohydrate/higher fat diets induced cardiovascular disease (Feinman et al., 2015). During the twentieth century, a popular hypothesis existed which suggested that high fat intake induced heart pathologies; more than a dozen studies that followed indicated that this supposition was not supported by evidence (Feinman et al., 2015). Conversely, it has been shown that excessive carbohydrate consumption can increase plasma lipid concentrations (i.e. dyslipidemia), as well as the likelihood of insulin resistance (Feinman et al., 2015).
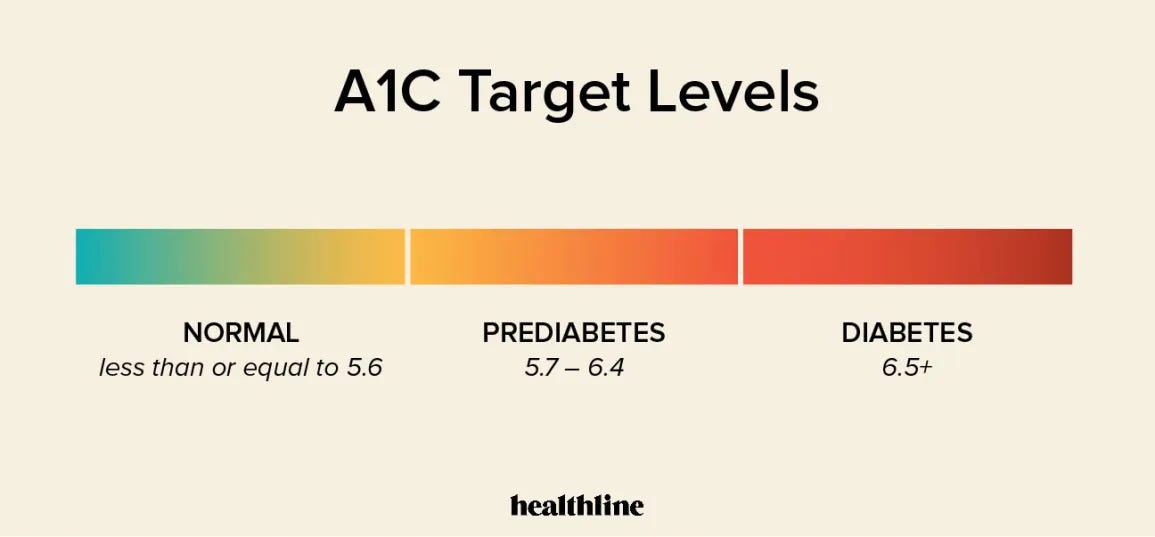
The ninth point of evidence to support the low carbohydrate protocol in diabetics is that the best predictor of microvascular complications is glycemic control (Feinman et al., 2015). HbA1c, an averaged measurement of blood glucose over two to three months, helps indicate how well diabetics manage their glucose levels (Feinman et al., 2015). Of particular interest, is that for every one percent reduction in HbA1c, there was a fourteen percent reduction in the risk of myocardial infarction (Feinman et al., 2015). Very low carbohydrate ketogenic diets (VLCKDs) have been shown to decrease HbA1c, a potential method of liberating a diabetic from exogenous insulin dependence (Feinman et al., 2015).
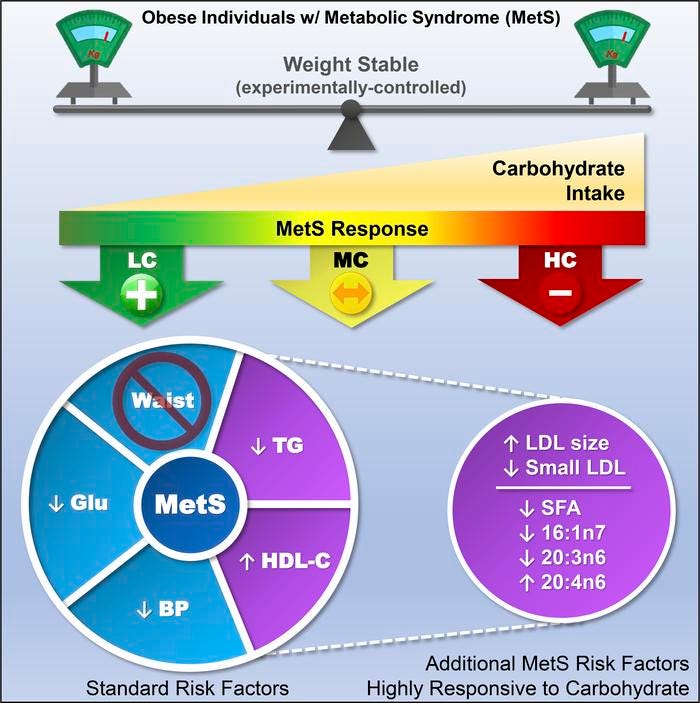
The tenth point of evidence stated that carbohydrate restriction is an effective method for reducing serum triglycerides, and increasing high-density lipoproteins (HDLs) (Feinman et al., 2015). Additionally, Feinman et al. (2015) compared low glycemic diets, high carbohydrate protocols, and their associated effects on HDLs. Evidence revealed that low glycemic diets raised HDLs more (1.7 mg/dL) than high carbohydrate diets (0.2 mg/dL). Additionally, low carbohydrate interventions decreased bodyweight and lowered blood glucose concentrations more than high carbohydrate diets (Feinman et al., 2015).

The eleventh, and perhaps most persuasive, point of evidence is that type 2 diabetic patients on carbohydrate restricted diets reduce and frequently eliminate medication, and type 1 diabetics usually require less insulin (Feinman et al., 2015). Medication and insulin reductions among diabetic individuals can be attributed to enhanced modulation of blood glucose levels elicited from low carbohydrate protocols. Furthermore, Feinman et al. (2015) noted, which is also intuitive, that such a reduction in medication for a diseased state, is commonly viewed as a sign of effectiveness in therapeutic contexts.
Finally, the twelfth point of evidence presented by Feinman et al. (2015) indicated that the intensive glucose lowering effects of carbohydrate restrictive diets have no side effects, as compared to pharmacologic interventions. This helps substantiate the safety and efficacy of this non drug-mediated intervention, and that belief of harm from nutrition-controlled diabetes management is but conjecture, and devoid of evidence (Feinman et al., 2015).
Several interventions have been proposed to manage diabetes. However, not all interventions are created equally. Although pharmacological interventions are sometimes necessary, they are not always required, and consumer vigilance dictates that we seek out alternatives, which provide maximum return, minimal risk, and minimal cost. Evidence suggests that low carbohydrate nutritional interventions can fulfill these requisites, liberating individuals from disease, and dependency on drugs.
References
Feinman, R. D., Pogozelski, W. K., Astrup, A., Bernstein, R. K., Fine, E. J., Westman, E. C., …Worm, N. (2015). Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base. Nutrition, 31(1), 1-13.
Giugliano, D., Ceriello, A., Razzoli, E., & Esposito, K. (2008). Defining the role of insulin lispro in the management of postprandial hyperglycaemia in patients with type 2 diabetes mellitus. Clinical Drug Investigation, 28(4), 199-207.
Paoli, A., Rubini, A., Volek, J. S., & Grimaldi, K. A. (2013). Beyond weight loss: a review of the therapeutic uses of very low-carbohydrate (ketogenic) diets. European Journal of Clinical Nutrition, 67, 789-796.
-Michael McIsaac