

Optimal gastrointestinal (GI) function is central to a strong immune system and overall health; it is the gateway between the outside environment and the delicate internal systems of the human body. Ultimately, dysfunction of the gut barrier can give rise to a host of maladies negatively affecting homeostasis. One such condition is known as celiac disease (CD). As a means of appreciating the GI system, the following will explore CD, its etiology, affects upon the human body, and treatment via nutritional modifications.
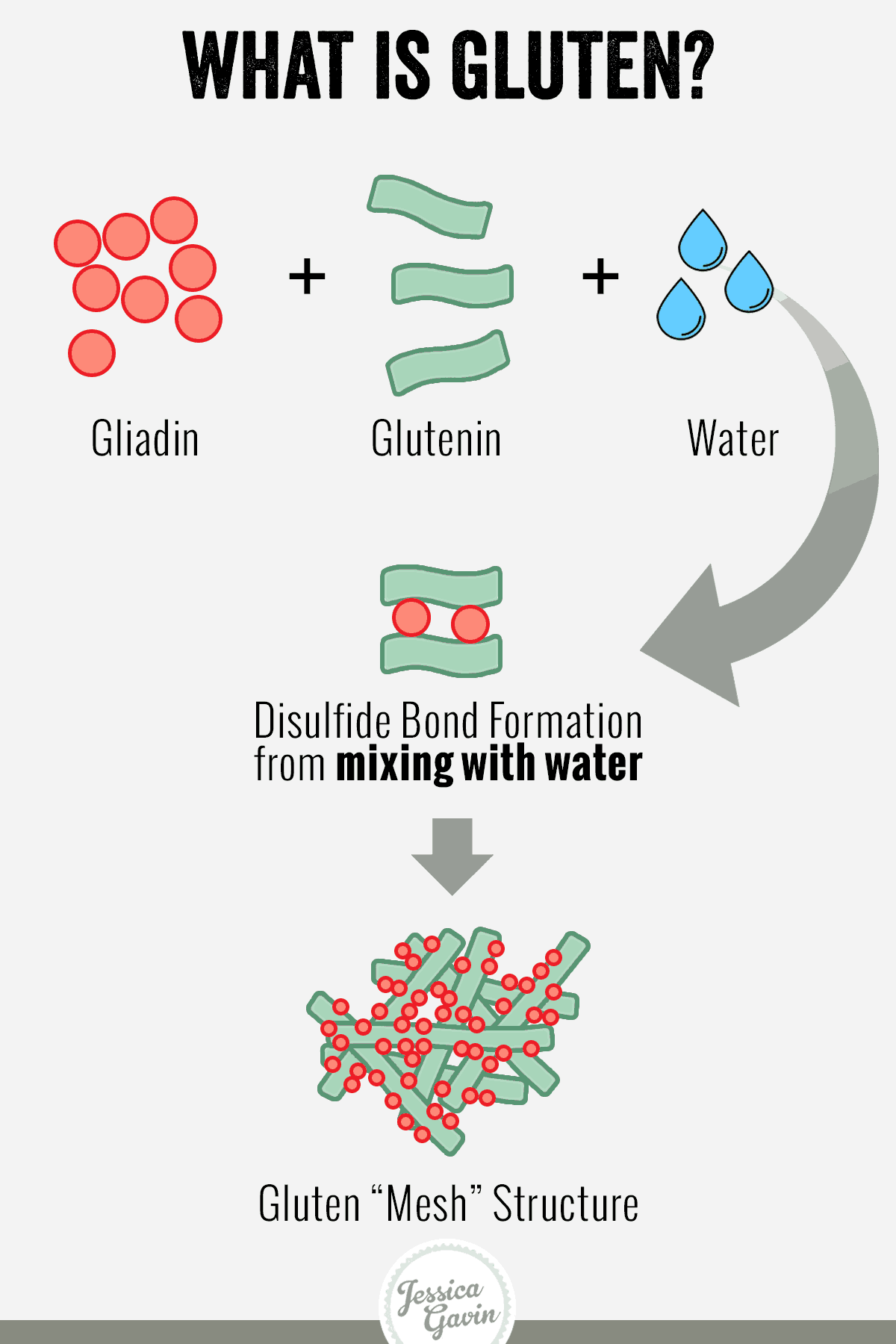
CD, also known as ornontropical sprue, celiac sprue, and gluten-sensitive enteropathy, is a common digestive disease affecting approximately 1% of North American and European populations (Chang, Burke, & Golub, 2011; Zimmer, 2011). Individuals suffering from CD are genetically predisposed and are reactive to foods containing a particular protein known as gluten (a storage protein found in wheat, barley, and rye) (Chan et al., 2011). Such reactions from gluten cause an immune-mediated systemic response, leading to inflammation and damage along the intestinal lining (i.e., inflammatory bowel disease). Symptoms include diarrhea, distended abdomen, failure to thrive, and abdominal complaints. Ultimately, CD leads to malabsorbtion of nutrients, which provides a gateway to other diseases, and further disrupts homeostasis (Zimmer, 2011).
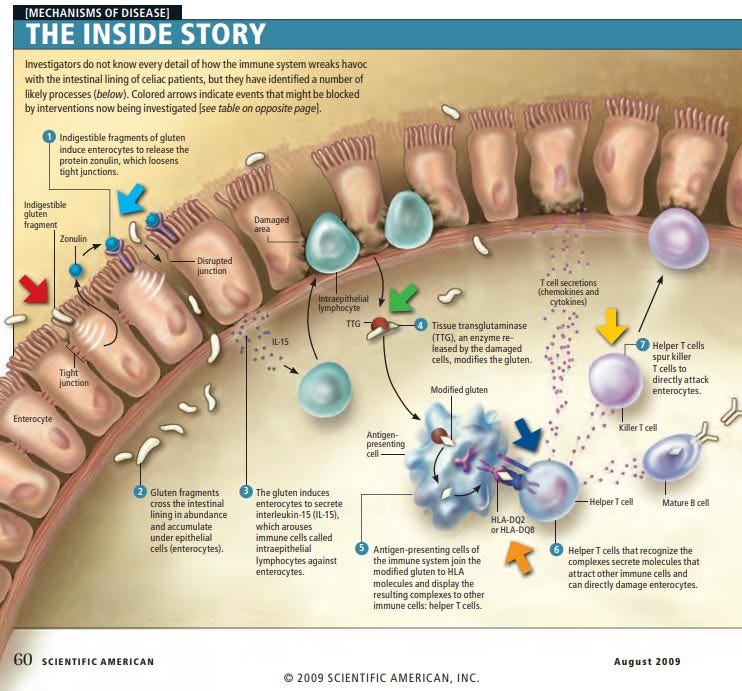
Reactivity to gluten occurs only in individuals that carry a human leukocyte (white blood cell) antigen known as HLA, and a potent immune response ensues involving both an innate and adaptive response (See, 2006). The innate portion of the immune system engages within hours after consumption of gluten including activation of the lymphocytes within the surface epithelium, changes/alterations in the epithelial cells producing certain cytokines (cell-signalling proteins involved in the immune response), specifically interleukin (IL)-15, which further activates the immune response to continued gluten exposure (See, 2006). Ultimately, such a response destroys the intestinal villi (structures, which absorb nutrients) changing the permeability of the intestinal lining (See, 2006).
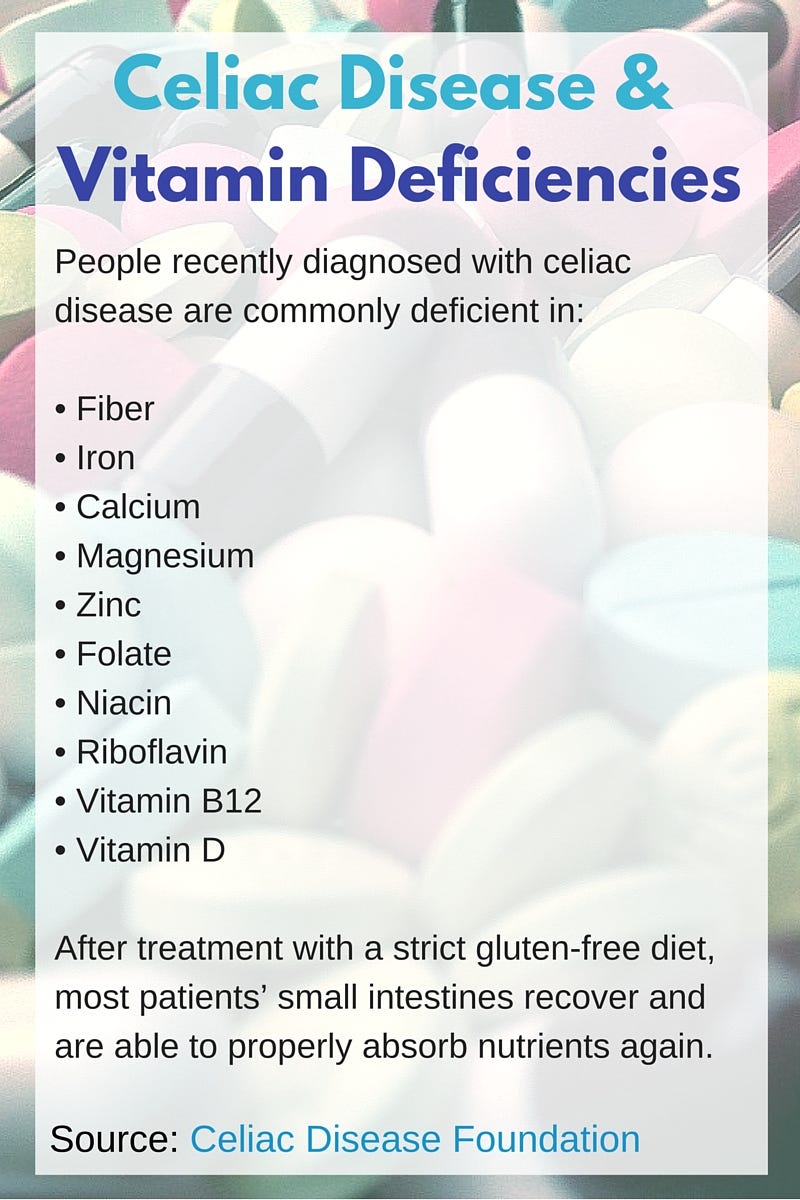
Such small intestinal alterations from celiac results in malabsorbtion of key nutrients such as iron and folic acid. Additionally, fat-soluble absorption is also reduced because of the compromised ability of the intestine to digest fats. Finally, vitamin B12 absorption is problematic in those with CD (See, 2006). Considering that gluten is the impetus behind the autoimmune response in CD, it is also reasonable to consider that removal of said protein in the diet would relieve an individual from further reactivity. See (2006) noted that complete removal of gluten in the diet can result in a substantial recovery from CD.

Cessation of gluten in those with CD can have dramatic improvements in the health and function of the villi, in addition to reductions in systemic inflammation and inflammation of the intestinal epithelium (See, 2006). However, the rate of recovery is dependent on compliance, age, and severity of the illness before gluten is removed (See, 2006). Of particular relevance is the degree of gluten-free nutrition compliance from an individual with CD; noncompliance can lead to increased morbidity and mortality in patients with CD due to associated conditions (See, 2006). Such conditions include infertility, skeletal disorders, and malignancy in addition to elevated health care costs; non-compliant individuals tend to see multiple subspecialists and undergo multiple tests and treatments (See, 2006). Most importantly, the mortality rate at every age is boosted in noncompliant patients (See, 2006). Thus, complete cessation of gluten ingestion is paramount to fully restore gut function and health.
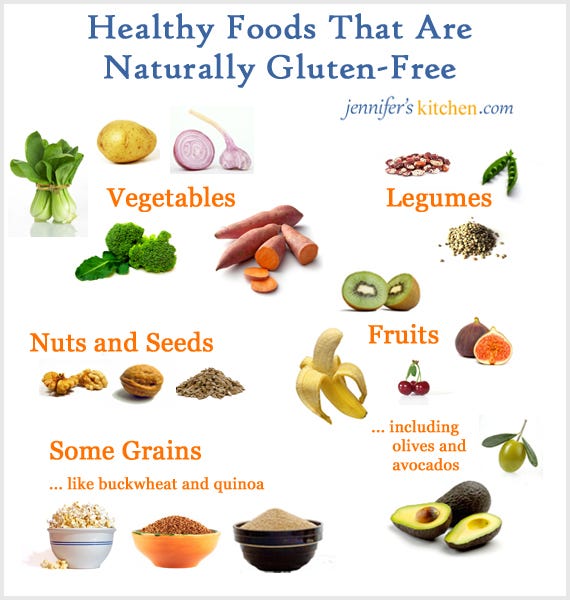
In conclusion, CD can be a debilitating disease, in addition to facilitating progression of other diseases from malabsorbtion of nutrients. However, solutions do exist that are both simple in their approach (excluding gluten in the diet) and cost effective. However, it is paramount that complete, and permanent, abstinence from gluten is achieved if individuals truly wish to liberate themselves from the illness.
References
Chang, H. J., Burke, A. E., & Golub, R. B. (2011). Celiac disease. The Journal of the American Medical Association, 306(14), 1614.
See, J. (2006). Gluten free diet: The medical and nutrition management of celiac disease. Nutrition in Clinical Practice, 21(1), 1-15.
Zimmer, K.P. (2011). Current problems in pediatric and adolescent health care. The American Journal of Medicine, 41(9), 244-247.
-Michael McIsaac