

Chronic diarrhea is also known as irritable bowel syndrome (IBS), with a predominant symptom of diarrhea (IBS-D). IBS-D is characterized by abdominal pain, diarrhea and abdominal discomfort. The pathogenesis may be linked to factors such as visceral hypersensitivity, brain-intestine axis disorders, intestinal flora alternations, and intestinal motility abnormalities.1(888) In the following sections, this author will consider common symptoms, their relationship to blood/urinary/stool biomarkers, and nutritional interventions to help manage and support recovery from IBD-D.

The four R program (FRP), as discussed in this author’s last post, is a useful and systematic means of addressing gastrointestinal dysfunction. FRP is characterized by: phase 1-removing allergenic foods and microbial overgrowth using bacteriostatic (slows bacterial reproduction)/mycostatic (slows fungal reproduction) agents, phase 2-replacing digestive enzymes, phase 3-reinoculating with favorable microbes, and phase 4-repairing gastrointestinal tissue and immune system integrity.2 As such, the following sections will outline biomarkers (i.e., urinary, blood, stool) while relating their presence and relevance to the FRP.

If an individual reported gastrointestinal discomfort while consuming particular foods, this author would recommend a food allergy test if available. If, for example, an individual’s food allergy test result indicated a moderate to high sensitivity (measured by IgG) towards casein (a protein found in milk and other dairy products) and yogurt, this author would recommend removal of the same from the diet. Such a step would represent phase 1 of the FRP. The second half of phase 1 would include reduction/removal of overpopulated and/or pathogenic microbes. As such, the following sections will explore the same.

If an organic acids test indicates a high concentration of D-lactate, this author would recommend steps to control the rise of said marker. D-lactate is a marker that, when high, can indicate poor digestion and absorption of dietary carbohydrates.2(384) Several strains of bacteria, to include Lactobacillus plantarum, that normally populate the human gut have the capacity of converting simple sugars into D-lactate; a metabolite of such a process. Left unmanaged, it is possible that D-lactate production can exceed clearance leading to lactic acidosis. Thus, removal of simple sugars in the diet could help control the production of D-lactate and associated symptoms. Finally, introduction of antibacterial agents such as berberine, citrus seed extract, and garlic can help control overgrowth.2(390)
If stool profiles indicate the presence of Bacteroides vulgatus, steps should be taken to control high concentrations of the same. Many strains of Bacteroides species convert bile to metabolites and fecapentaenes, which have been thought to be mutagens and/or co-carcinogens.3 Only two Bacteroides species, Bacteroides stercoris and Bacteroides vulgatus, showed significant association with such high risk.3(3205) Similarly, if stool analysis indicates overdominance of Pseudoflavonifractor spp., control of said bacteria might be indicated as it has been associated with colon cancer, likely due to its capacity to produce hydrogen sulfide; a substance involved in the pathophysiology of cancer.4 Finally, as was mentioned in the previous section, introduction of antibacterial agents such as berberine, citrus seed extract, and garlic can help control overgrowth.2(390)
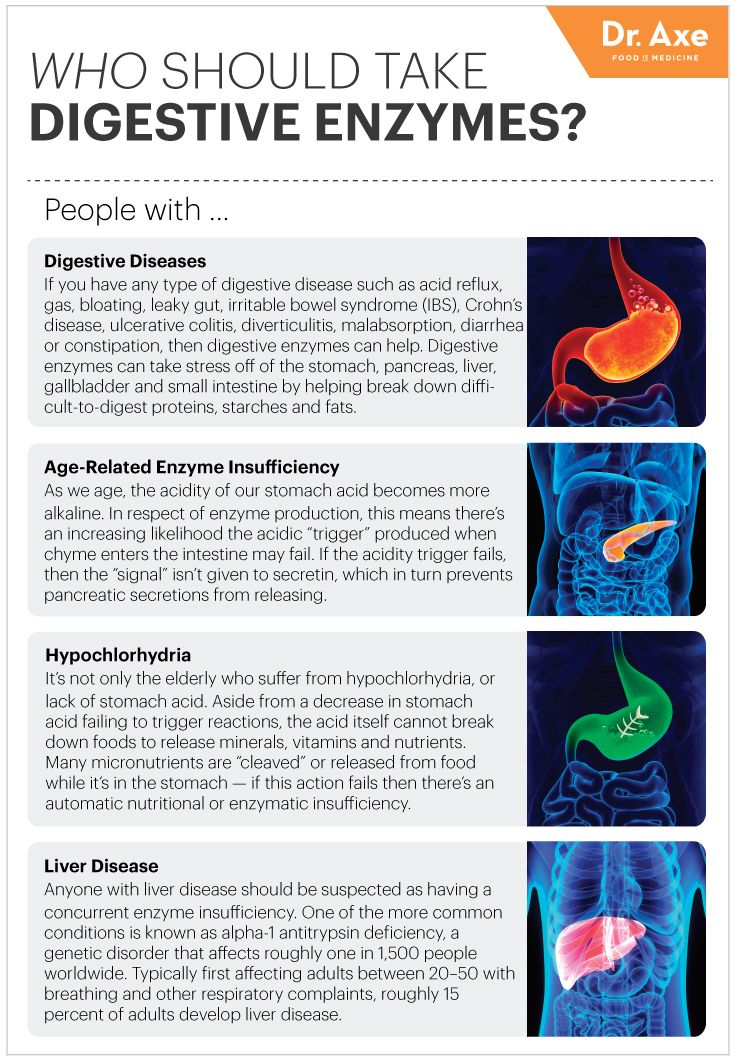
Phase 2 of FRP includes replacing digestive enzymes, if deficient. D-lactate concentrations not only rise from overpopulation of bacteria like Lactobacillus plantarum; poor digestion of carbohydrates is an often a precipitating factor.2(385) One stool test that could help elucidate digestive enzyme production could be the pancreatic elastase – 1 (PE1); an enzyme with high diagnostic sensitivity and specificity used in the diagnosis in pancreatic insufficiencies.5 If said enzyme is low/insufficient, this author would suggest implementation of oral pancreatic enzyme supplementation. Finally, this author would also consider analysis of stomach pH as poor acidity (i.e., high pH), also known as hypochlorhydria, has been found to reduce vitamin and mineral absorption/protein digestion, and has been implicated in food allergies.6 If stomach acidity is poor, supplementation with betaine hydrochloride might be indicated.
LINK: Pancreatic Enzyme Replacement Therapy
LINK: Optimizing Stomach Acidity With Betaine Hydrochloride
The third phase of FRP includes re-introduction of beneficial microbes when and where indicated. Probiotics are microorganisms which share a harmonious/symbiotic relationship with the gastrointestinal tract. Said microorganisms facilitate the prevention of diseases (i.e., inflammatory bowel disease, antibiotic associated diarrhea), modulate immune system function, enhance epithelial barrier function, and control the build-up of toxin-producing bacteria.7 Lord et al2(440,454-455) suggested implementation of favorable microbes and general dysbiosis using L. acidophilus, L salvarius, L. plantarum, L. casei, and Saccharomyces boulardii. However, if D-lactate markers are already high, this author would recommend against using additional exogenous L. acidophilus as it could worsen overpopulation.2(386)
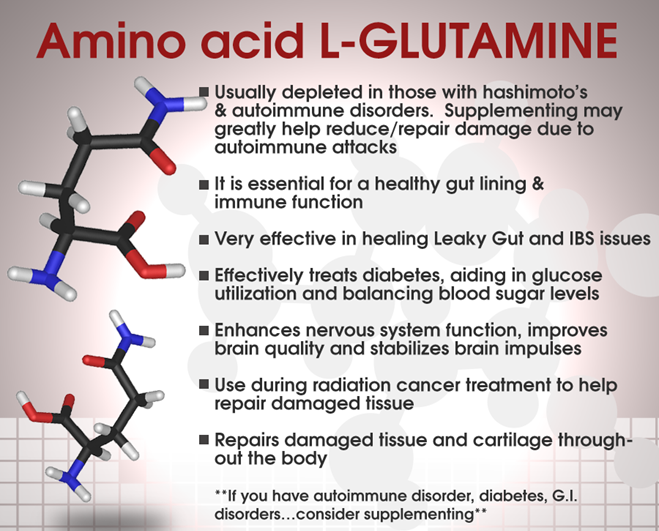
The fourth phase of FRP entails repair of the intestinal tract, especially if intestinal permeability is present. Such permeability can be measured by the lactulose/mannitol test covered in this author’s previous posts. If permeability is detected, implementation of glutamine can provide an energy source to facilitate/expedite the repair of intestinal tissue. If inflammatory markers are high (i.e., eosinophil protein X; which is highly associated with gut inflammation), essential fatty acids such as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) can also help remodel cell membranes/control inflammation along the intestinal wall in addition to supplementation of zinc, vitamin A/C/E, folic acid, pantothenic acid (B5), and free form amino acids to support cell growth and protection.2(455)8 During said phase, this author would also consider exposures to toxins and develop strategies to reduce said exposures, especially if organic acids such as 2-methylhippurate (indicates xylene exposure from building products/paint thinners/vehicle exhaust) and glucarate (marker of liver detoxification) are elevated.2(363-365)
In conclusion, IBS-D is characterized by abdominal pain, diarrhea and abdominal discomfort. The pathogenesis may be linked to factors such as visceral hypersensitivity, brain-intestine axis disorders, intestinal flora alternations, and intestinal motility abnormalities. Once IBS-D has been diagnosed, steps should be taken to remove foods, pathogenic microbes, and environmental exposures that could be contributing to said condition. Finally, introduction of digestive enzymes, beneficial microbes, essential fatty acids, amino acids, and other micronutrients that can help improve digestion, absorption, inflammation, and repair of the intestinal tract is critical. Such steps, especially when guided by FRP, can systematically support recovery from IBS-D and help liberate individuals from illness.
References
1. Zu-dong T, Sheng-sheng Z, Xiao-hua H, et al. Post-marketing evaluation of tongxiening granules in treatment of diarrhea-predominant irritable bowel syndrome: A multi-center, randomized, double-blind, double-dummy and positive control trial. Chin J Integr Med. 2019;25(12):887-894. doi:10.1007/s11655-019-3030-x.
2. Lord RS, Bralley JA. Laboratory Evaluations for Integrative and Functional Medicine. Duluth, GA: Genova Diagnostics; 2012.
3. Moore WEC, Moore LH. Intestinal floras of populations that have high risk of colon cancer. Appl Environ Microbiol. 1995;61(9):3202-3207. doi: 10.1128/AEM.61.9.3202-3207.1995.
4. Ai D, Pan H, Li X, et al. Identifying gut microbiota associated with colorectal cancer using a zero-infiltrated lognormal model. Front Micro. 2019;10:1-8. doi:10.3389/fmicb.2019.00826.
5. Amanquah SD, Darko R, Maddy SQ, et al. Fecal pancreatic elastase – 1: A non-invasive measure of exocrine pancreatic function. WAJM. 2004;23(3):240-244. doi: http://dx.doi.org/10.4314/wajm.v23i3.28130.
6. Pizzorno J, Katzinger, J.Clinical pathophysiology: A Functional Perspective. Coquitlam, BC: Mind Publishing Inc; 2012.
7. Khalighi AR, Khalighi MR, Behdani R, et al. Evaluating the efficacy of probiotic treatments in patients with small intestinal bacterial overgrowth (SIBO)- A pilot study. Indian J Med Res. 2014;140(5):604-608. http://www.ijmr.org.in/temp/IndianJMedRes1405604-481902_132310.pdf. Accessed March 2, 2020.8.
8. Peterson CGB, Sangfelt P, Wagner M, et al. Fecal levels of leukocyte markers reflect disease activity in patients with ulcerative colitis. Scand J Clin Lab Invest. 2007;67(8):810-820. doi:10.1080/00365510701452838.
-Michael McIsaac