
Post-rehabilitation (PR) clients require diligent and scrupulous program design. This population is often deconditioned and weak, decreasing the available margin of error and increasing the risk of re-injury. Thus, program development and the pursuit of best practice should be grounded in pragmatic and evidence-based approaches. In the following sections, I would like to explore evidence-based medicine (EBM), its utility in the health and fitness industry, and its affects upon my field of work.
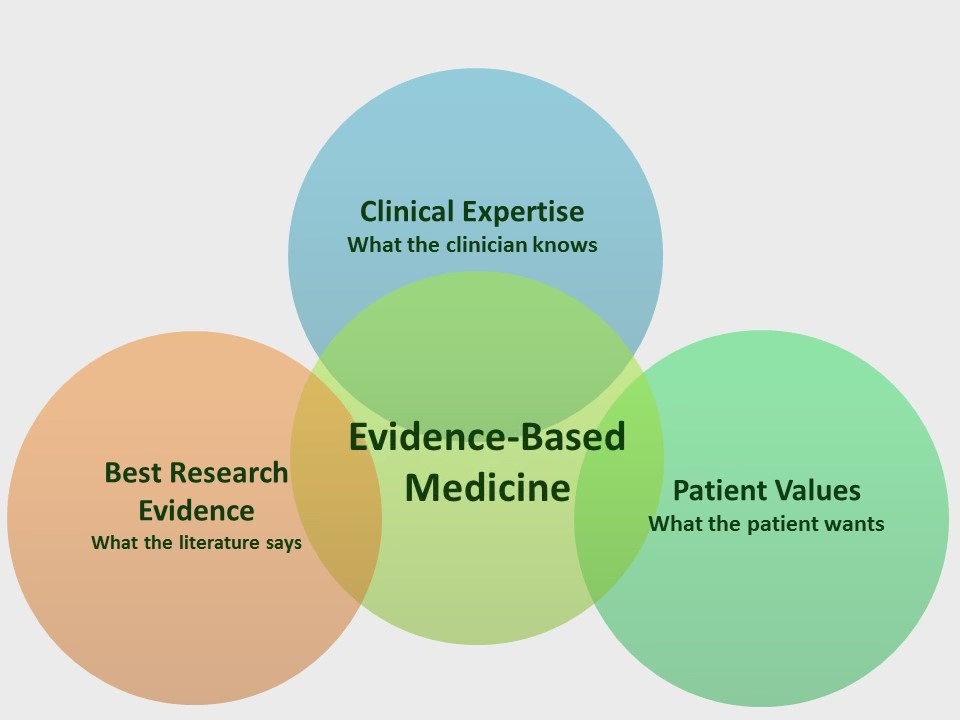
EBM can be defined as the tracking, critical appraisal, and implementation of evidence-based research into one’s own field of practice (Sackett & Rosenberg, 1995). EBM’s utility is seen more deeply within the medical field, as its genesis can be traced here (Sackett & Rosenberg, 1995). However, evidence based approaches can be, and are, used in other fields such as the exercise professional industry. Its importance and implementation can be supported in several ways.

EBM provides proven methods of creating some form of change as it is based on evidence, hence, evidence based medicine (Bazian Ltd., 2005). This allows us to use approaches that have been shown to make marked changes in a person’s health or fitness outcomes (i.e., improved strength, cardiac output, fat loss). EBM also helps establish credibility and legitimacy. In the exercise professional field, people can hold the title of exercise professional by ascertaining a weekend certification up to, and including, degrees from bachelors, masters, and Ph.D. levels in exercise science. This large stratification in knowledge and skill sets, with little-to-no higher requirements for entry into the industry, allows people to enter the field with lots of expertise, and little expertise. EBM can help provide a map for everyone to follow guidelines that are quick to access and easy to follow (Bazian Ltd., 2005).

In my field of PR, I try as much as possible, to fuse my experience with evidence-based practice. However, clinicians often do not implement EBM citing little time available for continuing education (Sackett & Rosenberg, 1995). In my work, I can devote 45-60 minutes of time per session. Moreover, I am not forced to create a solution after the first session, as the initial assessment is strictly an information-gathering opportunity. Thus, I can research the issue when necessary, and return during the next session with a well devised plan. Bazian Ltd. (2005) found that EBM couldhelp clinicians in their decision-making processes. However, clinicians cite restriction of available time as a limitation of EBM’s application. This outcome may be different with exercise professionals, as lower client ratios may provide more time for exercise professionals to engage in implementation of EBM.
If we wish to see the exercise professional industry to takes its place next to other older and more deeply rooted professions, we must take steps that establish it as a legitimate, professional, and credible field. EBM stands as an integral part of that overall process.
References
Bazian Ltd. (2005). Do evidence-based guidelines improve the quality of care? Evidence-Based Healthcare and Public Health, 9, 270-275.
Sackett, D. L., & Rosenberg, W. M. C. (1995). The need for evidence-based medicine. Journal of the Royal Society of Medicine, 88,620-624.
-Michael McIsaac