
INTRODUCTION
You know at least one grandparent, or perhaps one of your friend’s grandparents, who slowly shuffled around when you were a child. You might also remember how cautiously they moved when getting up from a chair or climbing the stairs. Back then, you probably thought it was normal part of aging. I am here to tell you that this does not have to be “normal” and there are interventions to manage these changes. Let’s learn a little more about this problem first, however.
TELL ME MORE?
In the context of aging, the ability to move around your environment freely (where you want, when you want, and how you want) is known as mobility.1 Some specific examples of mobility include using different types of transport (cars, buses), engaging in work and play, walking, or transferring from a bed to a chair.1(1508) As you can see, mobility is a pretty vital quality to have, and maintain.

HOW PREVALENT ARE MOBILITY ISSUES?
31.7% of adults 65 years and older have difficulty walking 3 city blocks, while another 20% of the same age group do not drive a car?1(1508) This is a problem for aging populations because these two basic methods of getting around (driving, walking) are important to access goods (i.e., food) and services (i.e., doctor visits, pharmacy visits) vital to maintaining health and wellness.1(1508)
I’m sure you can also imagine that a loss in mobility leads to sedentary behaviour; Satariano et al.1(1508) noted a lack of daily movement/exercise is independently associated with
- Depression
- Losses in cognitive function
- Breast cancer
- Colon cancer
- Diabetes
- Cardiovascular disease
- Obesity
Losing mobility also means individuals experience social isolation, which is also associated with a host of health conditions, including all-cause mortality (death from any cause).1(1508)
WHAT CAUSES LOSS IN MOBILITY?
It turns out that there are several culprits that drive mobility loss, and these include impairments in sensory systems, energy production, muscle/joint health, and neurological health.2 You can undergo tests such as walking speed over short distances, standing up from a chair/sitting back down, and balance tests to assess your degree of mobility loss.2(1185) These can tell you where you are, in early years, as a means of getting ahead of the problem. Although it is nice to have a read out of your abilities, let’s go deeper on the causes of mobility loss.
MOBILITY RISK FACTORS IN GREATER DETAIL
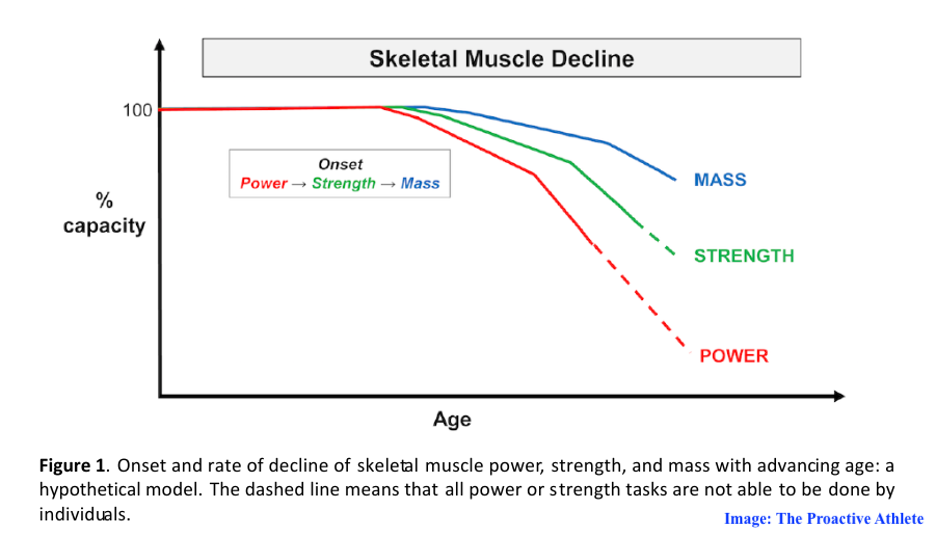
1. Body Composition and Strength: muscle mass is closely associated with muscle strength (the more you have, the stronger you are).2(1187) You gain lots of this in your early years, but around 60-70 years of age, you are likely to experience sharp losses in strength, and muscle mass.2(1187) Furthermore, high adiposity (i.e., fat on your body) deepens mobility losses over age. What we do know is that higher levels of strength in your early and mid-life helps protect you from disability in your advanced years.2(1188)
2. Energy Production: as you age, your aerobic capacity (i.e., cardiovascular fitness) declines.2(1188) In other words, performing the same task at an older age compared to younger years “takes more out of you.” This is because less oxygen (per breath) is making it from your lungs into muscles to help you make energy. This means you have to slow down so you don’t get winded.
3. Endocrine Dysregulation: this is fancy speak for describing problems with your hormones. Older individuals tend to experience difficulty managing glucose in their bodies. This leads to excessive glucose floating around and too much insulin; conditions known as hyperglycemia (too much glucose) and hyperinsulinemia (too much insulin).2(1189) To keep it simple, these lead to muscle loss over time, energy production issues, as well as chronic inflammation (you don’t want that).2(1189)
4. Nervous System: this is your “wiring” which allows messages to come from your brain and travel to many parts of your body, including your muscles. These nerves lose their coating (i.e., demyelination) over time, they also shrink (i.e., axonal atrophy), and as you age, it becomes more difficult to fix these issues.2(1189) Eventually, these nerve changes affect your senses, and contribute to strength losses, disability, and mobility impairments.2(1189) This also causes slow movement, changes in gait, and losses in balance.2(1189)

OK. HOW DO I FIX IT THOUGH?
You have been waiting patiently for this part of the article no doubt (thank you)! Let’s consider each of the risk factors previously mentioned above, one at a time:
1. Body Composition and Strength: You lose about 1% of strength per year after age 50, so let’s get cooking here.3 Simply put, you have to carefully progress towards lifting heavy (within >80% of a one repetition maximum) when weight training… if you want to increase strength/bone density.3(2) If you are worried that you will get hurt, research (~30 years) has consistently shown that heavy strength training is safe when weights are slowly progressed, and movements are slow and controlled.3(4) I would also suggest supervision from a Certified Kinesiologist, and a detailed medical history and movement assessment before you start. Think slow and steady 🙂
Article Link: Sarcopenia: The Importance of Exercise Selection and Stability
Article Link: Exploring Age-Related Strength Loss
Article Link: Strength Training and Sarcopenia
2. Energy Production: That feeling of “getting winded” is not so great. Strength is critical for conducting activities of daily living, but you also need to feed those muscles to keep going. Your heart and lungs need to be conditioned, and oxidative stress and low-grade chronic inflammation (learn more below) are not helping here.4 BUT, aerobic exercise (brisk walking) “fights” oxidative stress/low-grade chronic inflammation, helps dilate your blood vessels, and protects your mitochondria (generators in your cells that make energy).4(5) Sneaking in about 75-150 minutes a week of moderate (or higher) aerobic activity will help motor you along.4(8)
Article Link: Antioxidants and Tracking Oxidative Stress
Article Link: Mitochondria and Cardiac Health: Exploring the Connection
Article Link: Mitochondria and Relationships to Health
3. Endocrine Dysregulation: Mentioned earlier, aging is associated with high blood glucose, in addition to lowered testosterone in men, higher testosterone in women, and high cortisol levels (stress hormone)… just to name a few.2(1189) These conditions contribute to muscle loss and other problems. The good news is that lowering starchy carbs (article below) helps regulate blood glucose, insulin resistance, and inflammation.5,6 Furthermore, having extra muscle helps lower blood glucose (lift weights!) too.6(2) One last note; get your daily protein intake up. Protein is the ingredient for skeletal muscle, and amino acids (they make proteins)…make hormones!7
Article Link: Benefits of Very Low Carbohydrate Ketogenic Diets
Article Link: Essential Amino Acids and Why They Matter
Article Link: The Elderly: Optimal Protein Consumption and Sources
Article Link: Managing Elderly Diabetes: Carbohydrate Type and Fiber Consumption
4. Nervous System: It turns out that optimal vitamin D levels support neurological health and function (including mental health disorders).8 Consider supplementing everyday with vitamin D3 (1000 IU per 35 pounds bodyweight up to a maximum of 4000 IU of D3/day) especially if you live in northern latitudes. After 3 months, get your blood tested to see if your levels fall between 40-60 ng/ml.9 If it is still below 40 ng/ml, add 1000 IU of D3 and re-test in another 3 months. Oh, and make sure you are getting your omega-3 fatty acids in (i.e., fish oil). Optimal omega-3 fatty acid intake also supports neurological health and function. Optimal cell levels (i.e., omega-3 index) are between 8-12%.11 Consider supplementing up to 2000 mg/day, and test your levels in 3 months.10 If they are still below 8%, add 1000 mg and re-test in another 3 months.
Article Link: Vitamin D Supplementation: When, How, and Why?
Article Link: Nutritional Support for Traumatic Brain Injury
Article Link: Omega-3 Supplementation: Supporting Resistance Training and Recovery

CONCLUSIONS
So, there you have it. The ability to move around your environment freely is known as mobility, and you want to have LOTS of this in your golden years. But as you have seen, there are a few things you need to address to maintain your mobility, and make it better. Take things one step at a time, and seek out a qualified exercise professional and nutritionist to help motor you along. You WILL get your mobility back! Good luck 🙂
References
1. Satariano WA, Guralnik JM, Jackson RJ, Marottoli RA, Phelan EA, Prohaska TR. Mobility and aging: New directions for public health action.Am J Public Health. 2012;102(8):1508-1515. doi:10.2105/AJPH.2011.300631.
2. Ferrucci L, Cooper R, Shardell M, Simonsick EM, Schrack JA, Kuh D. Age-related change in mobility: Perspectives from life course epidemiology and geroscience.J Gerontol A Biol Sci Med Sci. 2016;71(9):1184-1194. doi:10.1093/gerona/glw043.
3. Tøien T, Berg OK, Modena R, Brobakken MF, Wang E. Heavy strength training in older adults: Implications for health, disease and physical performance.J Cachexia Sarcopenia Muscle. 2025;16(2):1-10. doi:10.1002/jcsm.13804.
4. Murray KO, Mahoney SA, Venkatasubramanian R, Seals DR, Clayton ZS. Aging, aerobic exercise, and cardiovascular health: Barriers, alternative strategies and future directions.Exp Gerontol. 2023;173:1027. doi:10.1016/j.exger.2023.112105.
5. Aloraini GF, McKeown NM, Rogers GT, Das SK, Lichtenstein AH, Jacques PF. Low-carbohydrate diet patterns that favor high-quality carbohydrates are associated with beneficial long-term changes in biomarkers of inflammation and oxidative stress in the framingham offspring cohort.Curr Dev Nutr. 2025;9(7):107479. Published 2025 May 28. doi:10.1016/j.cdnut.2025.107479.
6. Paoli A, Bianco A, Moro T, Mota JF, Coelho-Ravagnani CF. The effects of ketogenic diet on insulin sensitivity and weight loss, which came first: The chicken or the egg?.Nutrients. 2023;15(14):3120. doi:10.3390/nu15143120.
7. Gropper SS, Smith JL, Carr, TP. Advanced nutrition and human metabolism. 7thBoston, MA: Cengage Learning. 2018.
8. Barakat G, Yassine N, El Khoury N, Ramadan W. Vitamin D and brain health. Clin Nutr Open Sci.2026;67:1-31.doi:https://doi.org/10.1016/j.nutos.2026.100646.
9. CharoenngamN,Holick MF. Immunologic effects of vitamin D on human health and disease. Nutrients. 2020;12(7):1-28.doi:10.3390/nu12072097.
10. Krupa KN, Fritz K, Parmar M. Omega-3 fatty acids. Treasure Island (FL): StatPearls Publishing; https://www.ncbi.nlm.nih.gov/books/NBK564314/. Updated February 28, 2024. Accessed April 1, 2026.
11. Harris WS. Omega-3 fatty acids and cardiovascular disease: a case for omega-3 index as a new risk factor.Pharmacol Res. 2007;55(3):217-223. doi:10.1016/j.phrs.2007.01.013.