
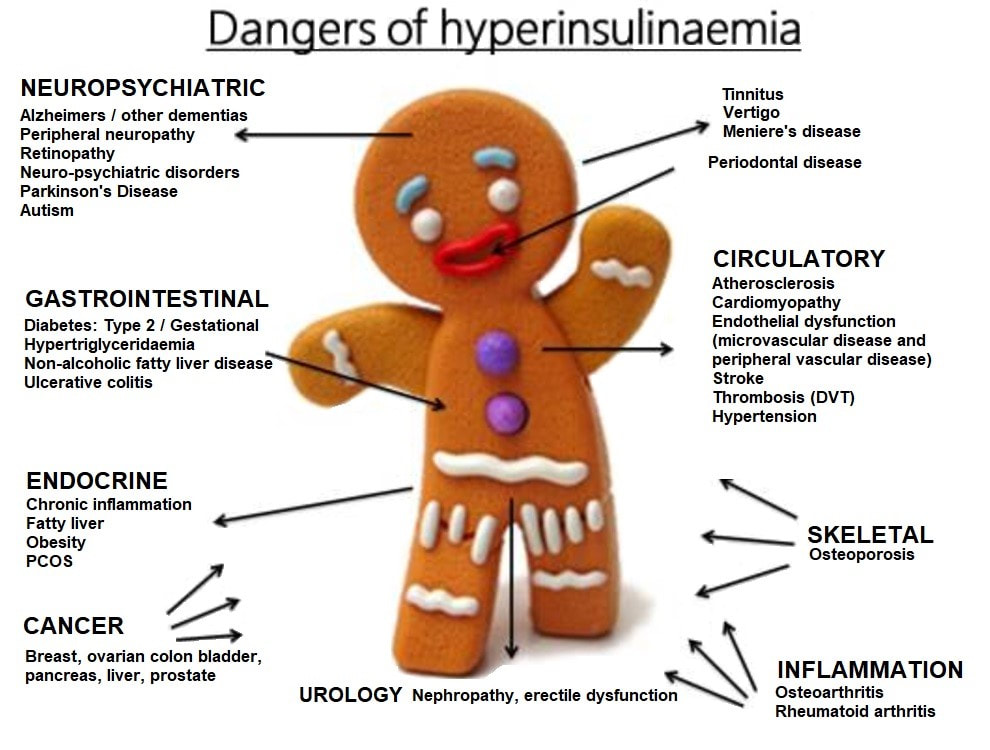
Insulin resistance (IR), a condition that effects 57 million people, is considered an early biomarker, and pre-cursor, of type 2 diabetes (T2D); a disease that currently effects 8% of the US population.2 IR is further characterized by high/normal levels of insulin, known as hyperinsulinemia (HI), required to dispose of blood glucose.1 Left unchecked, HI/T2D can worsen, inducing other disease states/conditions to include inhibited metabolism of carbohydrates/fats, pathologic changes in nerves/small blood vessels, and the development of atherosclerosis.3 As such, it is paramount to develop strategies that reduce hyperinsulinemia and IR, which includes modifications of nutrition. Thus, following will consider dietary approaches which support mitigation of HI/T2D.

Evidence suggested that most North Americans consume excessive levels of refined sugars in amounts exceeding 140 lbs, per year.4 Furthermore, said population derives 70% of calories from refined carbohydrate sources to include alcohol, vegetable oils, and sugar.5 Such nutritional habits drive an exaggerated postprandial insulin and glucose response, which stimulates further hunger and a perpetual overconsumption of added sugars and processed foods.4(38) Thus, if excessive sugar and refined carbohydrate consumption negatively affect normal insulin and blood sugar levels, it would be a logical approach to reduce the intake of such food sources. Such an approach is further supported by American Diabetes Association.6 The following will consider nutritional modifications for HI/T2D in greater detail.

Although American Diabetes Association6(S64) acknowledged that refined sugars and processed foods perpetuates the postprandial glucose/insulin response and ensuing hunger, said association believes that continued consumption of other complex starchy carbohydrate sources remain an important part of the diet. Such as assertion was based on the premise that complex carbohydrates contain an important source of energy, fiber, vitamins, and minerals.6(S64) Furthermore, American Diabetes Association6(S65) stated that no research has been conducted on individuals with T2D while restricting starchy carbohydrates to less than 130 grams/day. However, it should be noted that the American Diabetes Association6(S61) position statement was conducted in 2008.
More recent studies have elucidated findings that suggest low carbohydrate diets can have promising outcomes for individuals who are HI and who have T2D; Feinman et al7 stated that the benefits of carbohydrate restriction in T2D/HI were immediate and well documented. Furthermore, apprehensions regarding the safety and efficacy were conjectural rather than data driven. Feinman et al7 continued to outline that dietary carbohydrate restriction reliably lowered high blood glucose, did not require weight loss, and lead to a reduction or complete elimination of medications. Finally, low carbohydrate dietary interventions never indicated side effects, especially when compared to individuals who used drugs to manage HI/T2D.7(2)Please see the below link from this author outlining the benefits of low carbohydrate interventions in greater detail from Feinman et al7(2-10): https://www.mcisaachealth.com/insulin-resistance-type-2-diabetes-and-carbohydrate-restriction/
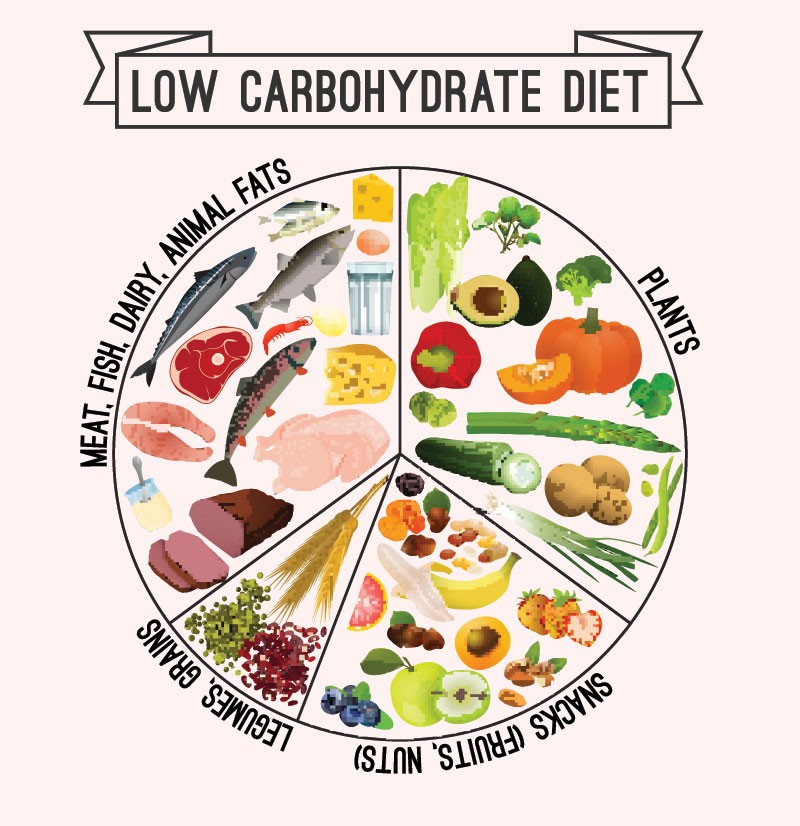
Cucuzella et al8 conducted a survey that was sent to individuals who have metabolic syndrome (to include HI/T2D). The majority of respondents (from a pool of 1580) had consumed less than 100 g of carbohydrates per day for over a year, most often for weight loss or disease management.8(1) Furthermore, the researchers noted that here was a reported decrease in weight and waist circumference concomitant decrease in hunger and increase in energy levels. Of the individuals who did provide laboratory reports and values, most individuals saw improvements in their hemoglobin A1C, lipid panels, and blood glucose measurements.8(1) Additionally, surveys indicated a reduction in usage of several medications, while 25% of the 1580 respondents reported medication cost savings of $288 per month for said respondents.8(1) Finally, the usage of pain relievers and anti-inflammatory medications dropped with simultaneous reductions in pain ratings and increases in mobility.8(1)
In conclusion, IR is a condition that effects 57 million people and is considered an early biomarker, and pre-cursor, of type 2 diabetes (T2D); a disease that currently effects 8% of the US population. Earlier evidence suggested that reductions in refined sugars would help manage HI/T2D. Additional, and more recent, research has helped substantiate such a position with further evidence supporting a general low carbohydrate dietary approach when managing HI/T2D. Ultimately, such approaches, especially when part of a larger and more inclusive intervention, should help liberate individuals from the downstream effects of excessive refined carbohydrate and sugar consumption.
References
1. Lord RS, Bralley, JA. Laboratory Evaluations for Integrative and Functional Medicine. 2 nd ed. Duluth, GA: Genova Diagnostics; 2012.
2. Hammaker BG. More than a coincidence: Could Alzheimer’s disease actually be a type
3 diabetes? J Diabetes Sci Technol. 28(9);2014:16-18. Retrieved from http://resolver.ebscohost.com.libproxy.bridgeport.edu/openurl?sid=EBSCO%3ac8h&genre=article&issn=10500758&ISBN=&volume=28&issue=9&date=20141101&spage=16&pages=16-18&title=Access&atitle=More+than+a+Coincidence%3a+Could+Alzheimer’s+Disease+Actually+Be+Type+3+Diabetes%3f&aulast=Hammaker%2c+Barbara+G.&id=DOI%3a&site=ftf-live
3. Lee RD, Nieman, DC. Nutritional assessment. 6 th ed. New York, NY: McGraw-Hill. 2013.
4. Anton SD, Martin CK, Han H, et al. Effects of stevia, aspartame, and sucrose on food intake, satiety, and postprandial glucose and insulin levels. Appetite. 2010;55(1):37-43. doi:10.1016/j.appet.2010.03.009.
5. Ilich JZ, Kelly, OJ, Kim Y, et al. Low-grade chronic inflammation perpetuated by modern diet as a promoter of obesity and osteoporosis. Arh Hig Rada Toksikol. 2014;65(2),139-148. doi: 10.2478/10004-1254-65-2014-2541.
6. American Diabetes Association. Nutrition recommendations and interventions for diabetes. Diabetes Care. 2008;31(1):S61-S78.
7. Feinman RD, Pogozelski WK, Astrup A, et al. Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base. Nutr. 2015;31(1):1-13. doi:http://dx.doi.org/10.1016/j.nut.2014.06.011.
8. Cucuzella MT, Tondt J, Docter NE, et al. A low-carbohydrate survey: Evidence for sustainable metabolic syndrome reversal. Journal of Insulin Resistance. 2017;2(1):1-25. doi: 10.4102/jir.v2i1.30.
-Michael McIsaac