
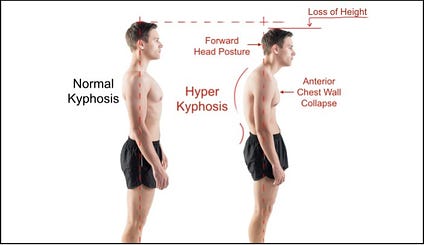
Non-invasive interventions exist to treat excessive kyphotic curves of the thoracic vertebrae (Katzman, Wanek, Shepherd, & Sellmeyer, 2010). However, these interventions prove futile in other cases. What then, causes this apparent loss in efficacy? I would like to review two predominant forms of kyphosis, their differences and implications, as well as their effects upon program design.

Postural kyphosis isattributed to poor posture, usually presenting with a smooth curve, which can be corrected by the client (Rothman Institute, 2013). This form of kyphosis can be managed by the modalities found in the work of Katzman et al. (2010). Structural kyphosis, however, is caused by abnormalities affecting the bones, discs, nerves, ligaments and muscles (Rothman Institute, 2013). Kyphosis with a structural cause may require medical intervention, as behavior modification and exercise will not restore normal curvature of the thoracic spine (Rothman Institute, 2013).
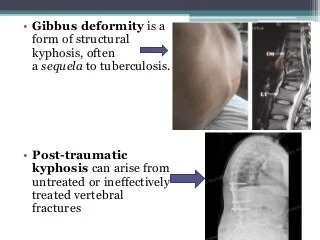
A specific type of structural kyphosis is a gibbus deformity. It is characterized by an abrupt and sharply angled change in the vertebral column, and is not a smooth curve (Rothman Institute, 2013). Another form of structural kyphosis is Scheuermann kyphosis. It is a hyperkyphosis defined by radiographic methods as an anterior wedging of ≥5° of at least three consecutive vertebral bodies(Wood, Melikian, & Villamil, 2012). This particular form of structural kyphosis can start as early as preteen years, and is usually diagnosed between 12-14 years of age. Considering the differences between postural and structural kyphosis, how will this influence program design?

An intelligent first step is to know what form of kyphosis a client has. If they are unaware, advising the client to seek medical insight would be prudent. If the client has structural kyphosis, most corrective strategies and self-mobilizations may not work. Performing movements that may cause forward flexion of the spine such as loaded deadlifting patterns and back squats may place both the thoracic and lumbar vertebral discs in an unfavorable position. If this is ignored, repeated loading in a flexed posture may cause a disc herniation in a posterior direction (McGill, 2007). Modifications in supine positions may also be advised, as thoracic flexion will leave considerable space between the client’s head and the floor. Bolstering the posterior side of the head with matting or a foam roll would be recommended to alleviate hyperextension of the cervical vertebrae. Loaded overhead reaching such as dumbbell presses may also be contraindicated, as the shoulder complex would have to move beyond normal ranges of flexion to sustain an adequate overhead position. Plyometric exercise may also be ill advised because of ground reaction forces placed through the hyperkyphotic spine.
Structural kyphosis requires medical intervention to restore normal, or near normal, thoracic curvatures. Exercise programs must also acknowledge the restrictions that structural kyphosis carries with it. Having this condition does not mean that health and fitness programs be avoided. If exercise professionals modify the program to reduce flexion and compressive loads to the spine, clients should experience all of the physiological and psychological benefits that movement provides.
References
Katzman, W. B., Wanek, L., Shepherd, J .A., & Sellmeyer, D. E. (2010). Age-related hyperkyphosis: Its causes, consequences, and management.Journal of Orthopaedic & Sports Medicine. 40 (6), 352-360.
McGill, S. (2007). Low back disorders: Evidence-based prevention and rehabilitation(2nd ed.). Windsor, ON: Human Kinetics.
Rothman Institute (2013). Retrieved December 24, 2013, from http://www.rothmaninstitute.com/specialties/conditions/kyphosis
Wood, K., Melikian, R., & Villamil, F. (2012). Adult scheuermann kyphosis: Evaluation, management, and new developments. Journal of the American Academy of Orthopaedic Surgeons, 20 (2), 113-121. doi: 10.5435/JAAOS-20-02-113
-Michael McIsaac