

In this author’s last post, low stomach acidity (high pH), micronutrient maldigestion/malabsorption, causes/symptoms of high pH, and solutions to mitigate such conditions were considered. However, low stomach acidity can induce systemic affects where other physiological disruptions occur along the gastrointestinal (GI) tract, to include gut dysbiosis (Pizzorno & Katzinger, 2012). As such, the following will briefly consider gut dysbiosis, other GI functions, their relationship to high pH, and pathophysiological manifestations of the same.
Hypochlorhydria not only hinders the GI tract’s ability to digest and absorb micronutrients such as chromium, copper, magnesium, manganese, potassium, selenium, vanadium, and zinc; high pH directly influences the population, balance, and function of microbial species from fungi, viruses, bacteria, and parasites (aka microbiota) within the small and large intestine (Gropper, Smith, & Carr, 2018;Lord & Bralley, 2012). The 16-foot-long GI tract’s lumen and mucosa are densely populated with said microbes, playing a diverse set of roles to include conversion of indigestible components of foods into co-factors and essential vitamins. Other, more recent, functions of the microbiome include antagonization of pathogenic bacteria, metabolization of toxins, modulation of tight junctions, and maintenance of immune homeostasis (Pizzorno & Katzinger, 2012).Ultimately, low stomach acid can negatively affect all of the GI tract’s said functions. As such, the following will consider examples of species and physiological processes affected by low stomach acidity.
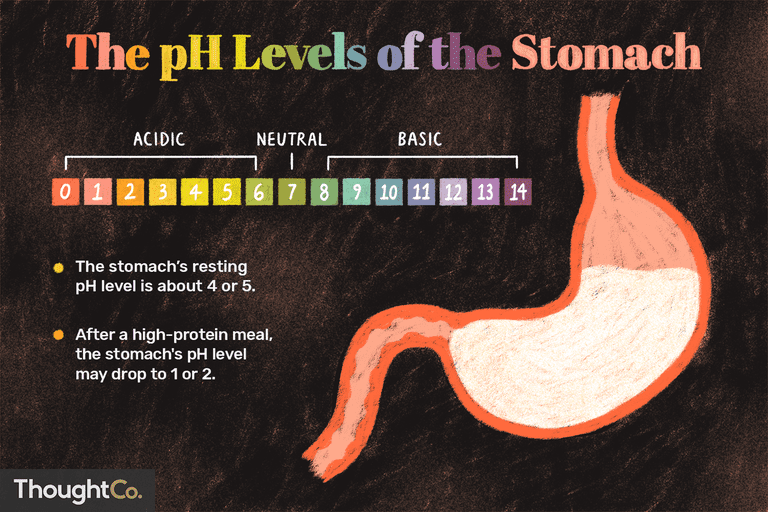
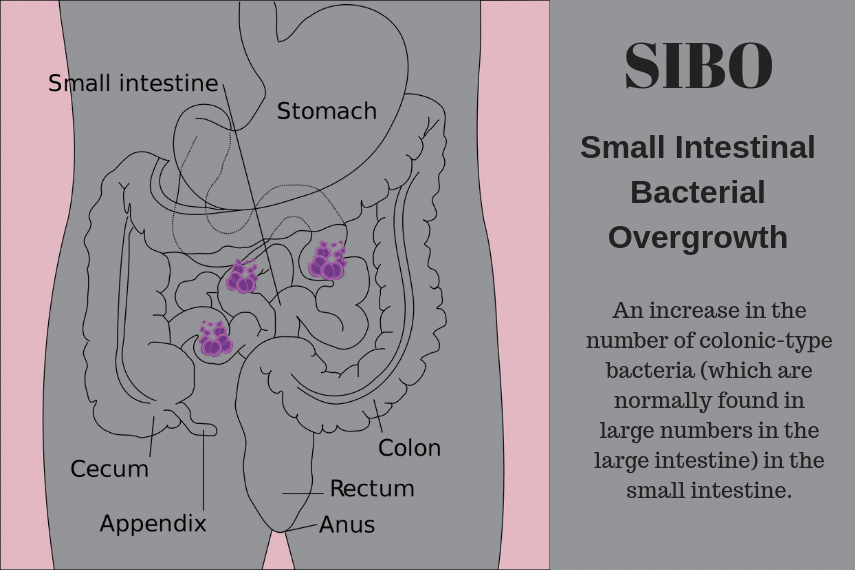
Gastric acidity was once believed to only affect stomach function. However, mounting evidence has supported the influence pH has upon the small and large intestine microbe colonies and function (Bavishi & DuPont, 2011). Gastric pH below 4 has a pronounced bactericidal affect, which generally kills exogenous bacteria found in food within a 15-minute period (Bavishi & DuPont, 2011). Conversely, stomach acid above a pH of 4 can potentially allow 50% of ingested bacteria to bypass the stomach. Furthermore, poor acidity allows the over colonization of residential bacteria that are otherwise controlled by low pH. Such an example would include C. difficile (CD); a bacterium, which produces toxins that induce intestinal inflammation and tissue death (necrosis) (Reisner & Reisner, 2017). Another example of disruption in gut function would include small intestinal bacterial overgrowth (SIBO). Such a condition can be induced by exogenous bacteria over colonizing the GI, or migration of microbes from the large intestine to the small intestine (Bavishi & DuPont, 2011). Left unchecked, SIBO can cause diarrhea, bloating, abdominal pain, anemia, weight loss, and malabsorption of nutrients.
In conclusion, hypochlorhydria not only causes maldigestion and malabsorption of micronutrients; its affects can be observed along the entirety of the GI tract. Over population of CD and the development of SIBO are only two examples (of several maladies) outlined to provide an appreciation of other side-affects associated with low stomach acidity. As such, awareness of stomach acidity and its systemic effects on GI function and overall health should be strongly considered; identification and appropriate management of hypochlorhydria is paramount if individuals present with high pH or other disease states associated with the same.
References
Bavishi, C., & DuPont, H. L. (2011). Systematic review: The use of proton pump inhibitors and increased susceptibility to enteric infection. Alimentary Pharmacology & Therapeutics, 34(11-12), 1268-1281.
Bruno, G., Zaccari, P., Rocco, G., Scalese, G., Panetta, C., Porowska, B., … Severi, C. (2019). Proton pump inhibitors and dysbiosis: Current knowledge and aspects to be clarified. World Journal of Gastroenterology, 25(22), 2706-2719.
Gropper, S. S., Smith, J. L., & Carr, T. P. (2018). Advanced nutrition and human metabolism(7thed.). Boston, MA: Cengage Learning.
Lord, R. S., & Bralley, J. A. (2012). Laboratory evaluations for integrative and functional medicine (2nded.). Duluth, GA: Genova Diagnostics.
Pizzorno J. & Katzinger, J. (2012). Clinical pathophysiology: A functional perspective. Coquitlam, BC: Mind Publishing Inc.
Reisner, E. G., & Reisner, H. M. (2017). An introduction to human disease: Pathology and pathophysiology correlations (10thed.). Burlington, MA: Jones & Bartlett Learning.
-Michael McIsaac