
Sears (2017) stated that heart disease, among other maladies, is a condition driven by inflammation. Sources of inflammation are widespread to include environmental (i.e., heavy metal exposure), lifestyle (i.e., sleep deprivation and stress), and nutrition (omega-6 rich processed foods) factors (Ilich, Kelly, Kim, & Spicer, 2014; Irwin, Olmstead, & Carroll, 2016; Umamaheswaran, Dasari, Yang, Lutgendorf, & Sood, 2018; Zheng et al., 2019). One intervention, among many, is to increase consumption of omega-3 fatty acids (O3FA) to mitigate inflammatory markers. As such, the following will explore said nutrient and its relationship to inflammation, and ultimately, cardiovascular function.
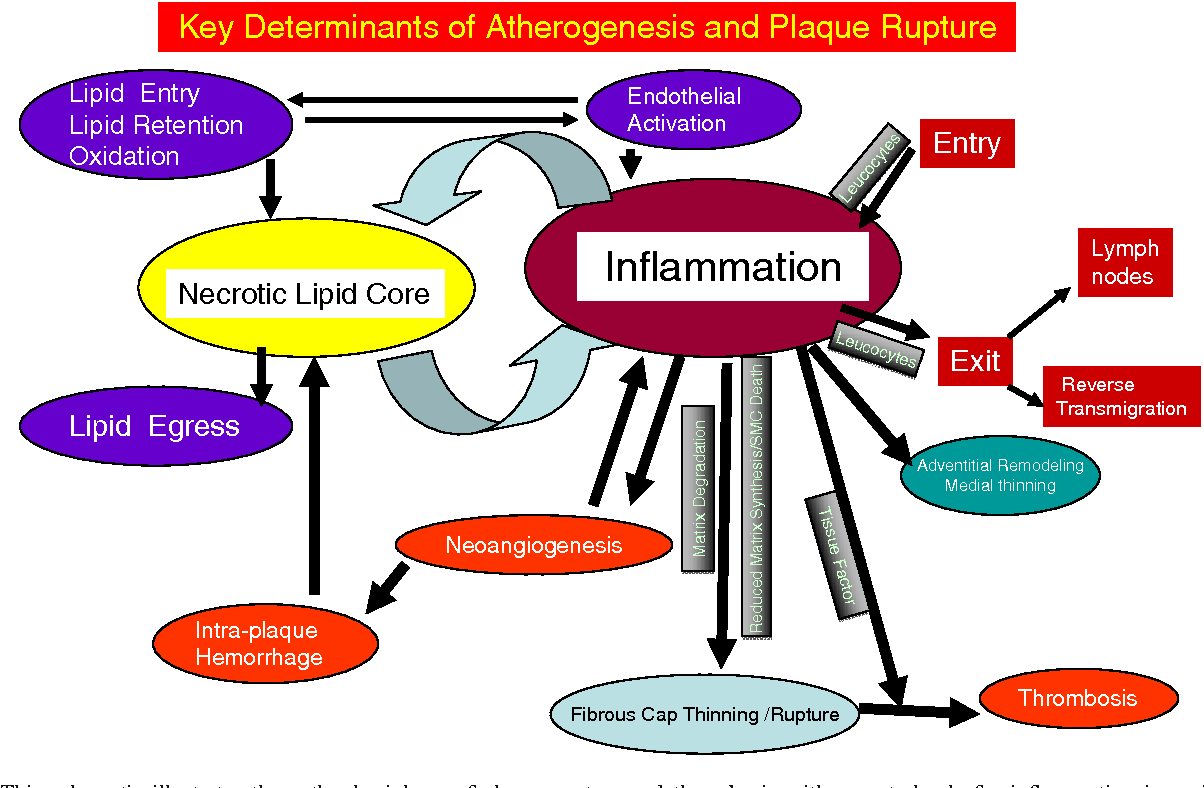
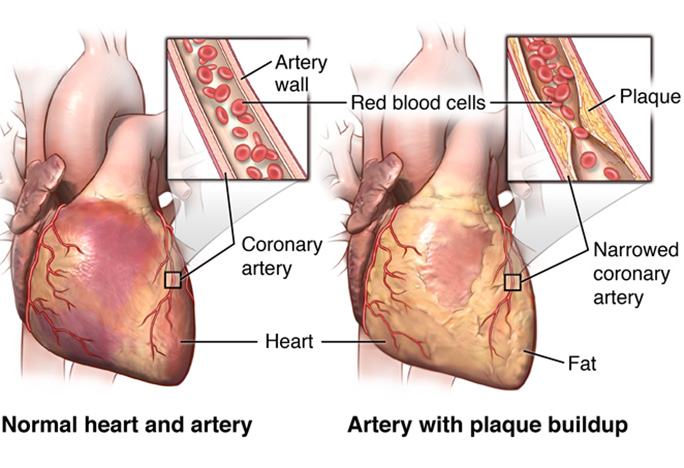
Coronary artery disease (CAD) is a condition characterized by a progressive thickening of fibrous plaques composed of abnormal cells, calcium, and cholesterol along the arterial walls supplying cardiac tissue (Basu, Pernecky, Sengupfa, & Liepa, 2006). Over time, said plaques tend to protrude into the lumen of the arteries reducing blood flow and oxygen supply and eventually inducing angina and myocardial ischemia. Such a condition exposes underlying collagen from within the endothelium, which aggregates platelets and eventually produces a thrombus. If the thrombus blocks a coronary artery, a heart attack occurs (Basu et al., 2006). Interestingly, inflammation is the underlying impetus behind disruption of the endothelium (Basu et al., 2006). Thus, it is paramount that interventions are implemented which prevent and/or minimize inflammation.
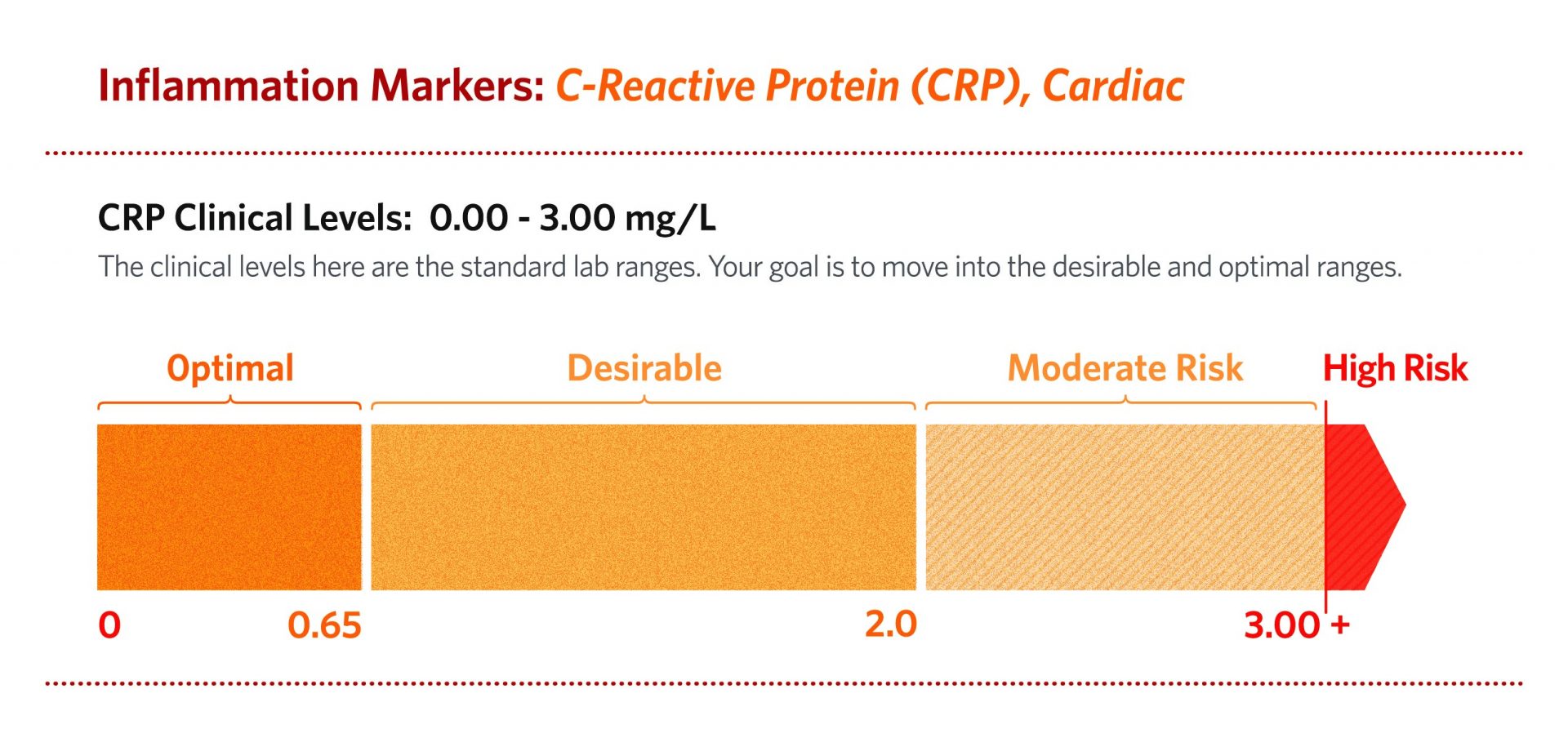
Several inflammatory markers increase as CAD progresses to include circulating interleukin-6 which controls the liver production of a substance known as C-reactive protein (CRP) (Basu et al., 2006). CRP is an acute-phase protein that generally flows at low levels but can become rapidly released from the liver; such an event can elevate CRP 1,000 times the normal level in the circulation in response to tissue injury, infection, and acute inflammation (Basu et al., 2006). Monitoring CRP levels is relevant because high levels are tightly correlated with cardiovascular disease risk factors such as triglycerides, total cholesterol, fibrinogen, and blood pressure. Most importantly, O3FAs can help mitigate underlying inflammation which drives the disease process behind CAD.

Basu et al. (2006) stated that several studies have supported O3FAs supplementation can play a preventative role in cardiovascular heart disease (CHD). One study referenced included 1015 males who ate two servings of fish per day while 1018 males were advised to avoid fish. After two years of said protocols, the fish-consuming group had a 39% reduction in all-cause mortality (Basu et al., 2006). Another study cited by Basu et al. (2006) contained 11,324 subjects with CHD who were randomized into a 850 mg O3FA group, 300 mg vitamin E group, both, or neither. After 3.5 years of following said protocols, the O3FA group showed a 45% reduction in sudden cardiac death and a reduction in all-cause mortality (Basu et al., 2006).

O3FAs are thought to exert their beneficial effects in several ways. One method of reducing myocardial infarction is through O3FA’s ability to reduce blood clotting capacity via down-regulating TXA2; a platelet aggregator and vasoconstrictor. O3FAs also up-regulates PGI; a vasodilator and platelet inhibitor (Basu et al., 2006). Another benefit of fish oil supplementation includes its ability to rapidly reverse carbohydrate-induced hypertriglyceridemia. Basu et al. (2006) indicated that O3FA supplementation (4 g/d) can increase catabolism of low-density lipoproteins (LDLs), decrease liver secretion of LDLs, and decrease further production of very low-density lipoproteins (VLDLs) and triglycerides in the liver. Such changes were achieved by 4 g/d of fish oil. O3FAs also helps reduce blood pressure; another risk factor for CAD. Basu et al. (2006) cited a meta-analysis of 36 studies supporting a reduction of systolic/diastolic blood pressure by an average of 2.1/1.6 mm Hg, respectively. The aforementioned changes were achieved by a median dosage of 3.7 g/d of fish oil (Basu et al., 2006).
In conclusion, CAD is an inflammatory condition driven by environmental, lifestyle, and nutritional factors. O3FA consumption, in doses between 3-4 g/d, appear to down regulate several degenerative processes affecting cardiac function. Although CAD is multifactorial, implementation of fish oil as part of a wider and more inclusive regime, can help minimize the chances of MI, thereby improving the health and longevity of at-risk individuals.
References
Basu, H., Pernecky, S., Sengupfa, A., & Liepa, G. U., (2006). Coronary heart disease: How do the benefits of ω fatty acids compare with those of aspirin, alcohol/red wine, and statin drugs? Journal of the American Oil Chemists’ Society, 83(12), 985-997.
Irwin, M. R., Olmstead, R., & Carroll, J. E. (2016). Sleep and inflammation: A systematic review. Society of Biological Psychiatry, 80(1), 40-52.
Ilich, J.Z., Kelly, O.J., Kim, Y., & Spicer, M.T. (2014). Low-grade chronic inflammation perpetuated by modern diet as a promoter of obesity and osteoporosis. Archives of Industrial Hygiene and Toxicology, 65(2), 139-148.
Sears, B. (2017). Commentary – Omega-3 fatty acids and cardiovascular disease: Do placebo doses give placebo results? Inflammation Research Foundation, 5(2), 1-4.
Umamaheswaran, S., Dasari, S. K., Yang, P., Lutgendorf, S. K., & Sood, A. K. (2018). Stress, inflammation, and eicosanoids; An emerging perspective. Cancer and Metastasis Reviews, 37(2-3), 203-211.
Zheng, X., Huo, X., Zhang, Y., Wang, Q., Zhang, Y., & Xu, X. (2019). Cardiovascular endothelial inflammation by chronic exposure to lead (Pb) and polycyclic aromatic hydrocarbons from preschool children in an e-waste recycling area. Environmental Pollution, 246, 587-596.
-Michael McIsaac