

In this author’s last post, Vladimir Janda’s lower crossed syndrome (LCS) and upper crossed syndrome (UCS) were explored, in addition to their relationships to the chronic musculoskeletal pain cycle (CMPC) (Page, Lardner, & Frank, 2010). Furthermore, mobility restrictions, one constituent of UCS and LCS, were covered as it related to the thoracic and hip regions, respectively.
As a means of appreciating mobility issues within UCS and LCS, expositions of normal anatomy, presentation of dysfunction, underlying causes, and assessments to measure joint range of motion were provided. In the following sections, motor control (also known as stability) a second constituent of UCS and LCS, will be explored including normal anatomy, presentation of dysfunction, underlying causes, and methods to assess dysfunction.
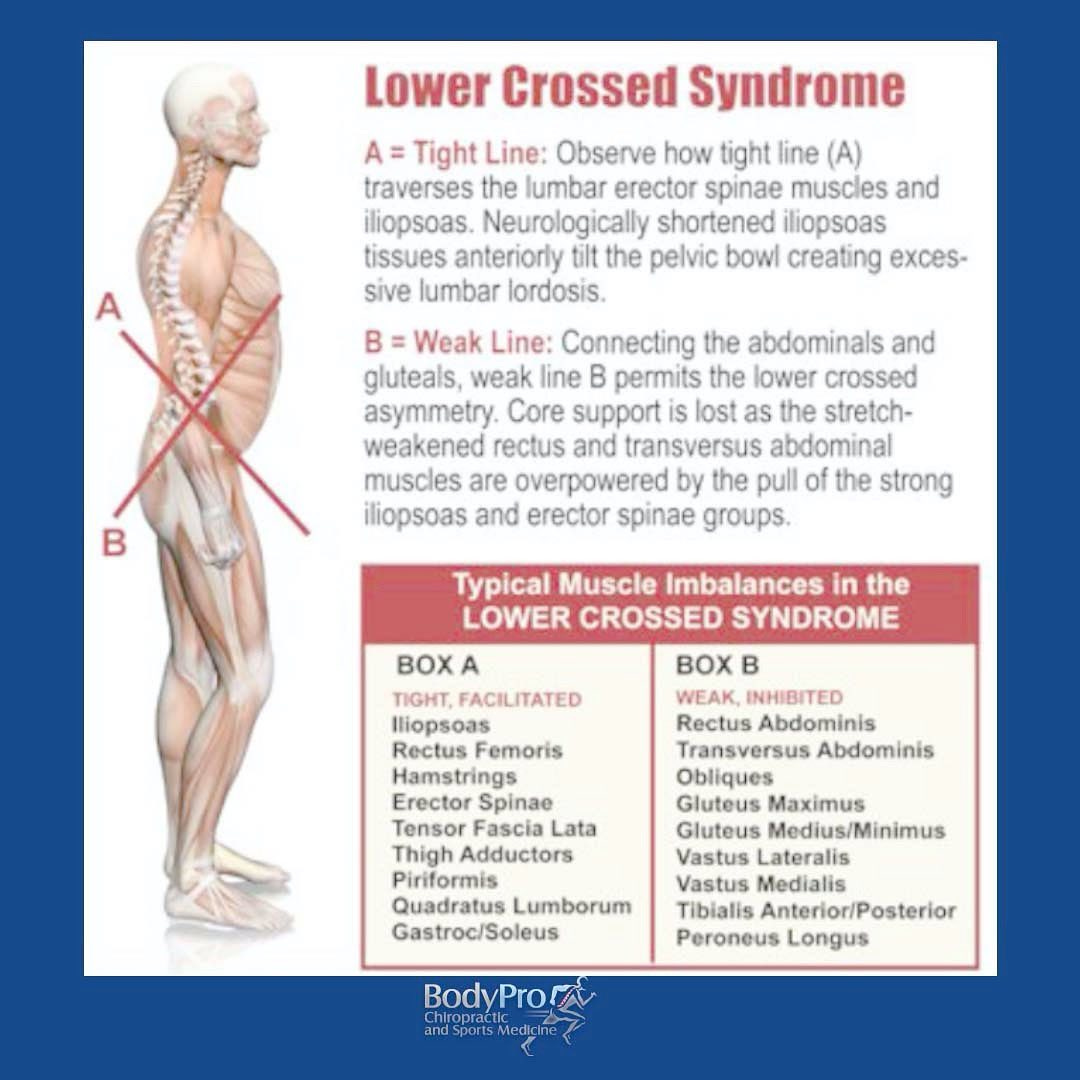
As described in this author’s last post, LCS is characterized by inhibited abdominals of the anterior side, in conjunction with the gluteus maximus/minimus/medius on the posterior side of the body (Page et al., 2010). The rectus femoris and psoas major of the anterior side, in conjunction with the thoraco-lumbar extensors of the posterior side, have a tendency to be overactive/facilitated (Page et al., 2010).
Such anomalies create a crossed pattern of facilitated and inhibited muscles (Page et al., 2010). This author also explained that the individual might present with low back pain; symptoms may increase when reaching overhead, standing, or lying supine with the legs extended (Sahrmann, 2002).

Hip stability/LCS, and functional strength in general, are rarely tested in absolute isolation (i.e., manual muscle testing) because many muscles (i.e., prime movers, synergists, stabilizers) work together to produce motion (Page et al., 2010). Although there exists value in testing force production of individual muscles, how and when they activate within the fabric of a complex pattern is of greater importance, as all of the aforementioned constituents produce motion (Page et al., 2010). Thus, methods, which assess functional strength should acknowledge such physiological proclivities.

Page et al. (2010) proposed the prone hip extension (unilateral) movement pattern test to assess hip stability. Within this test, the sequencing and degree of activation of the hamstrings, gluteus maximus, spinal extensors, and shoulder musculature are observed (Page et al., 2010). Proper sequencing of hip extension would include: hamstrings followed by the gluteus maximus followed by the contralateral erector spinae followed by the ipsilateral erector spinae (Page et al., 2010). Thus, any permutation of the aforementioned pattern would be considered faulty.
A common aberration would be over-activation of the hamstrings/erector spinae and delayed/absent contraction of the gluteus maximus (Tateuchi, Taniguchi, Natsuko, & Noriaki, 2012). The worst outcome would include initiation of hip extension by the erector spinae or shoulder musculature (Page et al., 2010). Such patterns would be clinically observed by a prominent anterior pelvic tilt with lumbar hyperlordosis as the client extends the hip. Other observations, which would help confirm faulty sequencing and activation would include hypertrophy of the hamstrings and erector spinae, in conjunction with atrophy of the gluteus maximus (Page et al., 2010).

In this author’s last post, UCS was characterized by crossed relationship between the upper posterior and anterior regions of the torso. The levator scapulae and upper trapezius on the posterior side tended to be facilitated, in conjunction with the pectoralis minor and major on the anterior side. Conversely, the serratus anterior and lower trapezius on the posterior side tended to be inhibited, in addition to the deep cervical flexors of the anterior side (Page et al., 2010).
This author also noted that winged scapula could stem from UCS, and the movement impairment could become pronounced during extension and flexion of the arms (Sahrmann, 2002). The aforementioned crossed patterns also drive the thoracic spine into hyperkyphosis, limiting extension and rotation (Page et al., 2010). Thus, a person with UCS may present with pain in the anterior shoulder area, as slouched posture is associated with shoulder impingement syndrome (Hamid-Rather, Riaz, Arshad, & Ahmed, 2014). Finally, the aforementioned symptoms may increase with overhead activities (Sahrmann, 2002).
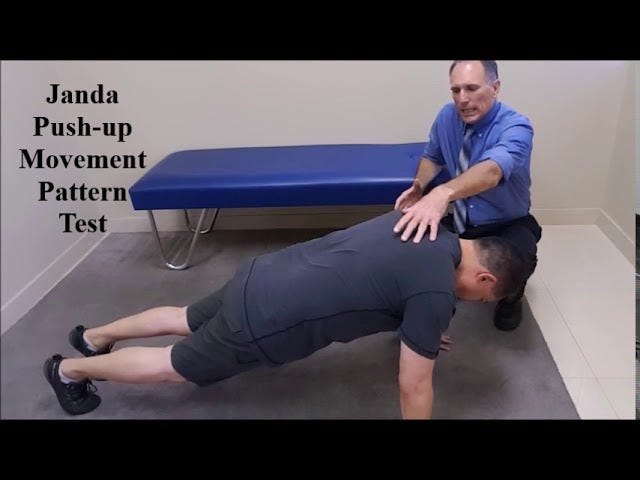
Page et al. (2010) proposed the push-up movement pattern test to assess the quality of dynamic scapular stabilization, one deficiency often found within UCS. Here, the client assumes a typical push-up position with legs extended. Once the client is in position, he/she begins to raise the body up from the floor. Proper sequencing and activation of serratus anterior and lower trapezius muscles (i.e., a force-couple) would allow the scapula to smoothly upwardly rotate with no scapular elevation (Page et al., 2010).
Thus, any permutation of the aforementioned pattern would be considered faulty. A common dysfunction, known as winged scapula, occurs via weakness of the serratus anterior and over-dominance of the levator scapula and trapezius; during the push-up, the scapula elevates and lifts away from the ribcage (Page et al., 2010). Scapular rotation, tipping, and abduction/adduction may also be present. Other observations to help confirm poorly stabilizing scapulae would include excessive bulk of the pectoral muscles (Page et al., 2010).
Proper movement is a complex and highly orchestrated event. The aforementioned stability tests are by no means a thorough or complete examination UCS and LCS. Rather, they are intended to provide brief insight and appreciation into the complexity and intricacies of human movement, and human movement dysfunctions. In conclusion, if one wishes to solve movement impairments, it is paramount to identify and deconstruct the mechanisms of optimal movement first. Only then can meaningful interventions follow.
References
Hamid-Rather, A., Riaz, S., Arshad, S., & Ahmed, S. (2014). Relationship of scapular position to shoulder muscle function: A comparative study between normal subjects and subjects with chronic protracted shoulders. JK-Practitioner, 19(3-4), 80-84.
Page, P., Lardner, R., & Frank, C. (2010). Assessment and treatment of muscle imbalances: The Janda approach. Champaign, IL: Human Kinetics.
Sahrmann, S. (2002). Diagnosis and treatment of movement impairment syndromes (1rst ed.). St. Louis, MO: Mosby Inc.
Tateuchi, H., Taniguchi, M., Natsuko, M., & Noriaki, I. (2012). Balance of hip and trunk muscle activity is associated with increased anterior pelvic tilt during prone hip extension. Journal of Electromyography and Kinesiology, 22(3), 391-397.
-Michael McIsaac