

In recent posts, I have covered omega-3 oils and their benefits. In recent years, a particular form of omega-3 (krill oil) has been researched and promoted for its particular health benefits. Such benefits include reduced hyperlipidemia, inflammation, and arthritis (Kwantes & Grundmann, 2015). As such, the following will consider krill oil, its safety, and comparative benefits to fish oil.

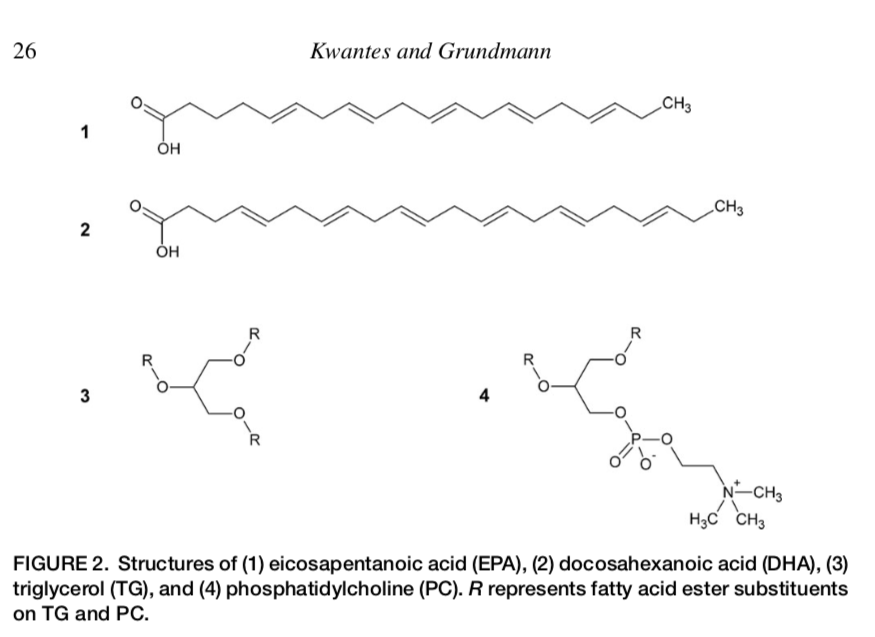
Krill are small crustaceans, also known as Antarctic krill, that reside in abundance (an estimated 300,000 million metric tons) along the Antarctic Ocean (Kwantes & Grundmann, 2015). Much of the research, as indicated by Kwantes and Grundmann (2015), has been focused upon the content and form of polyunsaturated fatty acids (PUFAs) found in krill oil; eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). As mentioned, EPA and DHA are both omega-3 fatty acids; EPA is a 20-carbon chain fatty acid identified as 20:5 (n − 3) and DHA is a 22-carbon chain fatty acid and is identified as 22:6 (n − 3) (Kwantes & Grundmann, 2015). However, EPA and DHA exist within regular fish oil as triglycerides (Kwantes & Grundmann, 2015).
Krill oil is thought to be particularly advantageous because its DHA and EPA are not found in triglyceride form. Rather krill oil’s PUFAs are bound to phospholipids in a form known as phosphatidylcholine (PC) (Kwantes & Grundmann, 2015). Such a structure is thought to contribute to the health benefits of krill oil (please see chart below). Additionally, claims have been made that less EPA and DHA from krill oil is required to receive the same benefits from higher doses of EPA and DHA from fish oil. Kwantes and Grundmann (2015) cited a study whereby 113 research participants which were divided into 3 groups comparing the health biomarkers of fish oil and krill oil. The following will explore the same.
During the 7-week krill oil Vs fish oil study, one group (36 participants) was given 3.0 g/day of krill oil, (supplying 543 mg of EPA + DHA), the second group (40 participants) was given 1.8 g/day of fish oil (providing 864 mg of EPA + DHA), while the third group received no supplementation (37 participants) (Kwantes & Grundmann, 2015). Results indicated a significant increase in plasma concentration of EPA and DHA from baseline compared to the control group.
Interestingly, there was no difference in plasma EPA and DHA between the krill oil group and the fish oil group, yet the amount of krill oil used was 62.8% of the total amount of EPA + DHA compared to the fish oil group (Kwantes & Grundmann, 2015). Such evidence might indicate the efficiency of krill oil over fish oil. A proposed theory behind such efficiency might be that the PC form of krill oil does not require bile salts to digest compared to fish oils, and PC might enter cells with more ease (because cellular membranes have a phospholipid layer) as they do not require a carrier mechanism (Kwantes & Grundmann, 2015).

In conclusion, krill oil appears to be more efficient, requiring smaller dosages to receive the same outcomes as fish oil. Of particular relevance is the sheer abundance of krill oil in the sea, which should allow new markets to develop, procure, and sell krill oil. Finally, krill oil might be a better alternative for individuals suffering from gall bladder/bile production pathologies as it does not require digestive salts to become absorbed, due to its hydrophilic qualities.
References
Kwantes, J. M., & Grundmann, O. (2015). A brief review of krill oil history, research, and the commercial market. Journal of Dietary Supplements, 12(1), 23-34.
-Michael McIsaac