
National Health and Nutrition Examination Survey has determined that approximately 0.9% of children between 1-5 years of age from 2005-2008 have lead blood levels surpassing 10mcg/dL (Brown, 2014). Due the toxic side affects of lead upon human physiology, it is paramount to control said lead levels.
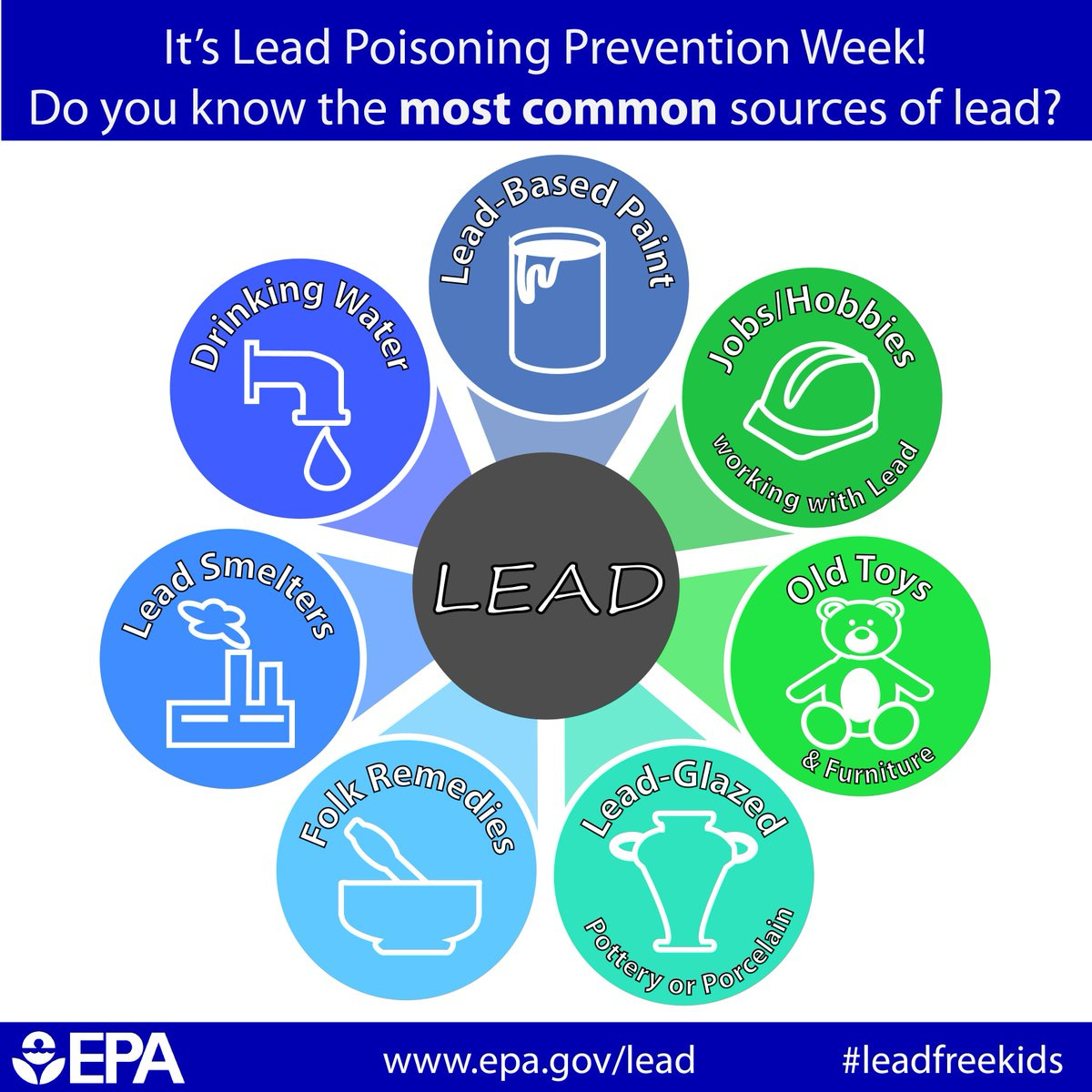
Common sources of lead exposure include airborne sources, although such sources have decreased since the elimination of lead from gasoline (Brown, 2014). Another significant means of lead exposure includes oral ingestion, as toddlers tend to place objects in their mouths (Brown, 2014). Furthermore, approximately 25% of children continue to live in homes that contain lead-based paint, as homes built prior to 1978 were likely to have said paints (Brown, 2014). Water piping is another source of lead exposure, as solder (contains lead) has been used to fuse lengths of piping. Some canned goods also contain lead, as it is used to fuse the ends of the items (Brown, 2014).
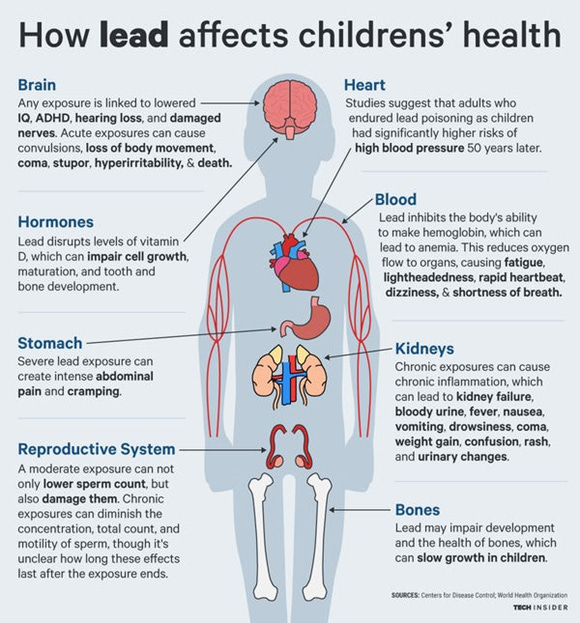
At exceedingly high levels, lead is an abortifacient when blood concentrations are >10ug/100ml. In males, blood levels of 5-9 ug/100ml has been linked to low libido, low semen volume, low sperm counts, and low sperm motility (Gildow, 2015). In children, acute encephalopathy (brain damage) occurs at concentrations of 80-100ug/100ml. Symptoms of said exposure includes irritability, agitation, headaches, confusion, drowsiness, convulsions, and coma (Gildow, 2015). Finally, some researchers indicated that for every 10ug/100ml exposure, there was a decrement of 4-7 IQ points (Gildow, 2015). In essence, there is likely no safe level of exposure to lead.

Considering the ubiquity of lead sources and its unfavorable affects on homeostasis, screening of said heavy metal is paramount. As such, screening is recommended at 9-12 months of age and 24 months of age when blood lead levels are known to peak (Gildow, 2015). Interestingly, many of the risk factors for lead toxicity are similar to iron deficiency anemia (older homes, living in poverty, sibling who has high lead levels) (Gildow, 2015).
Evidence suggests that treating iron deficiency anemia (IDA) may help mitigate the negative affects of lead exposure, in addition to increasing ingestion of vitamin C, although there is no strong evidence for such. However, vitamin C is still a relevant micronutrient in the diet as it helps mitigate IDA (Gildow, 2015). Additionally, evidence suggests that adequate calcium ingestion is paramount as it competitively decreases lead absorption. However, no research suggests that levels beyond adequate intake provide additional benefit (Gildow, 2015).
References
Brown, J. E. (2014). Nutrition through the life cycle (5th ed.). Stamford, CT: Cengage Learning.
Gildow, D. A. (2015). Lead toxicity. Occupational Medicine, 65(5), 348-356.
-Michael McIsaac