
Low carbohydrate diets (LCDs) have demonstrated favorable effects on biomarkers such as reduced triglycerides, total cholesterol, and improved insulin sensitivity (Ballard et al., 2013). However, do LCDs improve biomarkers as well as performance outcomes compared to grain-based diets (GBDs)? A case study by Rosenkranz, Cook, and Haub (2007) explored this question by placing an elite triathlete on two different dietary interventions, over two fourteen-day periods. One dietary intervention was composed of a LCD protocol (independent variable) consumed for fourteen days, followed by a blood profile (dependent variable) and a VO2maxtest (dependent variable) on a cycle ergometer. A rest period of three days separated the two protocols, whereby the participant could eat ad libitum.
Three days later, the participant commenced the GBD protocol (independent variable) for fourteen days. Again, a blood profile (dependent variable) and a VO2maxtest (dependent variable) on a cycle ergometer were performed. Comparison of post-intervention results indicated that the LCD produced: higher total cholesterol (178 mg/Dl compared to 160 mg/Dl from the GBD), elevated high-density lipoproteins (HDLs) (60 mg/Dl compared to 53mg/Dl from the GBD), elevated low-density lipoproteins (LDLs) (98 mg/Dl compared to 83 mg/Dl from the GBD), higher ratings of perceived exertion (17.2 compared to 14.8 from the GBD), higher resting heart rate (47.8 beats/min compared to 47.0 beats/min from the GBD), and a lower VO2max(67.3 ml/kg/min compared to 67.8 ml/kg/min from the GBD) (Rosenkranz et al., 2007). In the following sections, this author would like to look more deeply into the research methods of (Rosenkranz et al., 2007)as a means of determining the quality and applicability of the authors’ findings to the general population.
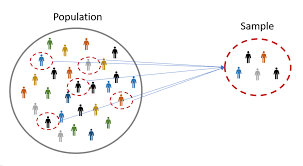
Sample size can be defined as the number of research participants in a sample for a particular study (Baumgartner & Hensley, 2006). Although sample sizes can be variable, Baumgartner and Hensley (2006) noted that the sample size doesbecome important when making inferences from the results of the sample to the population. Thus, the intervention study by Rosenkranz et al. (2007) had a sample size of one participant, making the applicability and external validity to the greater population, questionable.

As indicated in the aforementioned sections, post-intervention results in the VO2max were lower in the LCD protocol when compared to the GBD protocol. However, the difference was 0.5 ml/kg/min between both protocols; such a small disparity questions how meaningfully different the results were. Additionally, total calories between the LCD and GBD were not isocaloric in nature; the average caloric intake from the LCD was approximately 3736 kcal/d while the GBD was 3949 kcal/d, a resultant difference of 213 kcal/day (Rosenkranz et al., 2007).
Finally, when reviewing the three-day ad libitum diet between the two fourteen day protocols, pertinent questions arise; does the three-day ad libitum protocol represent the participant’s proclivities when not consuming a structured diet for an experiment? If so, the LCD protocol macronutrient ratios (21% carbohydrate, 23.5% protein, 54.7% fat) are radically different from the ad libitum diet (68.9% carbohydrate, 12.0% protein, 19.1% fat) as well as daily caloric intake (LCD was 923 kcal/d less than ad libitum diet) (Rosenkranz et al., 2007). Thus, It is possible that the participant may have required more time to acclimate to the new LCD protocol, beyond the fourteen-day limit.
Another limitation to the case study of Rosenkranz et al. (2007) was that of experimental control. Baumgartner and Hensley (2006) described control in experimental research as a means of monitoring and adjusting the effect of all variables, except the experimental variable. In an ideal situation, the researcher would control all aspects of the participant’s environment such as the amount of sleep, drug use, stimulation, stress, exercise, practice, and food intake (Baumgartner & Hensley, 2006). In the research of Rosenkranz et al. (2007), LCD and GBD foods were provided to the participant in pre-determined macronutrient proportions (LCD: 21% carbohydrate, 23.5% protein, 54.7% fat, GBD: 59.2% carbohydrate, 12.2% protein, 28.6% fat).
LCD foods consisted of chicken, fish, eggs, peanuts, beef jerky, cheddar-cheese, mozzarella, canned tuna, and canned ham. GBD foods included fruit, bread, pasta, rice, potatoes, whole-wheat tortillas, oatmeal, waffles, and breakfast bars (Rosenkranz et al., 2007). However, the participant did not live in the laboratory during the experiment; instead, logs were used to record food intake (Rosenkranz et al., 2007). It is possible that the food logs were inaccurate, thereby allowing the possibility of omitted food choices, and erroneous macronutrient ratios. Such potential errors would directly affect the internal validity (i.e., were conclusions based on the wrong information?) as well as external validity (i.e., to what extent was the information from the intervention applicable to the general population if the internal validity was questionable?).
A fourth limitation of the LCD/GBD intervention of Rosenkranz et al. (2007) was related to the order of the interventions; did implementing the LCD protocol first, followed by the GBD intervention, affect the outcomes for both? Research has indicated the effects of LCDs on cellular physiology; low carbohydrate intake can improve insulin sensitivity (Rosenkranz et al., 2007). Thus, it is possible that implementing the LCD protocol first may have augmented the effects of the GBD by enhancing the participant’s ability to metabolize glucose in a more efficient manner. Additionally, research supports that LCD interventions can increase glycogen storage levels when an individual returns to a higher carbohydrate diet (Burke, 2010). Thus, it is conceivable that the participant in the study of Rosenkranz et al. (2007) enhanced his glycogen storage capacity by initiating the LCD first. Such an increase in glycogen content may have facilitated the slightly higher VO2max scores and lower rates of perceived exertion during the second intervention on the GBD.
In conclusion, the case study by Rosenkranz et al. (2007) had several limitations. However, awareness of the weaknesses can provide an opportunity for vigilance when developing future research experiments. In this way, research continually refines and builds upon itself, leading researchers closer to certainty, and ultimately, the truth.
References
Ballard, K.D., Quann, E.E., Kupchak, B.R., Volk, B.M., Kawiecki, D.M., Fernendez, M.L., …. Volek, J.S. (2013). Dietary carbohydrate restriction improves insulin sensitivity, blood pressure, microvascular function, and cellular adhesion in individuals taking statins. Nutrition Research, 33(11), 905-912.
Baumgartner, T.A., & Hensley, L.D., (2006). Conducting and reading research in health and human performance (4thed.).New York, NY: McGraw-Hill.
Burke, L.M. (2010). Fueling strategies to optimize performance: Training high or training low? Scandinavian Journal of Medicine & Science in Sports, 2(20), 48-58.
Rosenkranz, R.R.,Cook, C.M., & Haub, M.D.(2007). Endurance training on low-carbohydrate and grain-based diets: A case study. Journal of Sport Nutrition and Exercise Metabolism, 17(3), 296-309.
-Michael McIsaac