

The scope of this author’s post is intended to address lumbar spine instability via corrective exercise and reinforcement interventions. However, it is essential to acknowledge and address the influence of distal regions (upper crossed syndrome and lower crossed syndrome) and their influence on proximal regions such as the lumbar spine, by way of regional interdependence (RI) (Sueki, Cleland, & Wainner, 2013). For posterity and programming effectiveness, it is assumed that UCS and LCS are addressed before, or in tandem with, lumbar spine instability. Having considered RI and its relationship to the lumbar spine, the following will explore the nature of low back pain, reinforcement methodologies, and exercise progressions to mitigate lumbar spine instability.
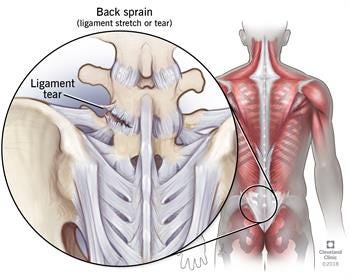
Lumbar spine tissue failure, instability, and pain are closely associated with specific loading and duration parameters; lumbar segments exposed to relatively low loads repetitively and/or sustained loads for long durations are precursors of injury (McGill, 2007). In essence, tissue failure occurs when the applied load is greater than the tissue strength (McGill, 2007). Such a scenario degrades motor control, endurance, and strength along the low back. Poorly stabilized abdominal muscles and hips have also been associated with low back pain (McGill, 2007). Cumulatively, both neuromuscular aberrations can feed into the chronic musculoskeletal pain cycle (CMPC) worsening the injury (Page, Lardner, & Frank, 2010).
After a medical professional has mitigated pain along the client’s low back (in this scenario), and has been cleared to work with this author, an initial consultation and functional movement screen would be performed. Below is a synopsis of such a client (referred to as Ms. F):
Ms. F reported being a moderately active 45-year old female (i.e., home-based yoga and line dancing) several days of the week. However, she is currently unable to participate in jogging, as it aggravates her lower back from a motor vehicle accident sustained in 2015. Subjective complaints included radiating pain (i.e., sciatica as reported by Ms. F) in Ms. F’s lower left back regions, in additional to numbness in the left foot. Ms. F reported that her upper back/shoulder/neck regions were weak and painful initially after the accident. However, the degree of pain and discomfort in said regions is considerably less intense at the time of this consultation and assessment.
During Ms. F’s movement screen, limitations were found in 5 of 7 fundamental movement patterns (Trunk Stability Push-Up, Overhead Squat, Shoulder Mobility, Active Straight Leg Raise, In-Line Lunge). Below is a synopsis of Ms. F’s movement screen:
| Screen (L=Left, R=Right) | Score (3=Excellent, 2=Average, 1=Needs Improvement, FN=Functional Non-Painful, FP=Functional Painful, DN=Dysfunctional Non-Painful, DP=Dysfunctional Painful) |
| Active Straight Leg Raise L | 1 |
| Active Straight Leg Raise R | 1 |
| Shoulder Mobility L | 2 |
| Shoulder Mobility R | 3 |
| Thoracic Spine Mobility L | ~45 Degrees |
| Thoracic Spine Mobility R | <45 Degrees |
| Neck Extension | FN |
| Neck Flexion | FN |
| Neck Rotation L | FN |
| Neck Rotation R | DN |
| Active Impingement Shoulder Test L | – |
| Active Impingement Shoulder Test R | – |
| Rotary Stability L | 2 |
| Rotary Stability R | 2 |
| Flexion Pain Test | – |
| Trunk Stability Push-Up | 1 |
| Extension Pain Test | – |
| In Line Lunge L | 1 |
| In Line Lunge R | 1 |
| Hurdle Step L | 2- |
| Hurdle Step R | 2 |
| Overhead Squat | 1 |
| Ankle Mobility L | 2” |
| Ankle Mobility R | 2” |
| Diaphragmatic Breath | Poor |
| Regions of Muscle Tenderness | Hips, Mid-Back, Rotator Cuffs |
As mentioned in the aforementioned sections, thoracic and hip mobility/stability deficits would be worked upon first before placing heavier emphasis upon the core regions of Ms. F. Corrective exercises chosen to improve Ms. F’s low back stability and endurance will be explored in the following sections.
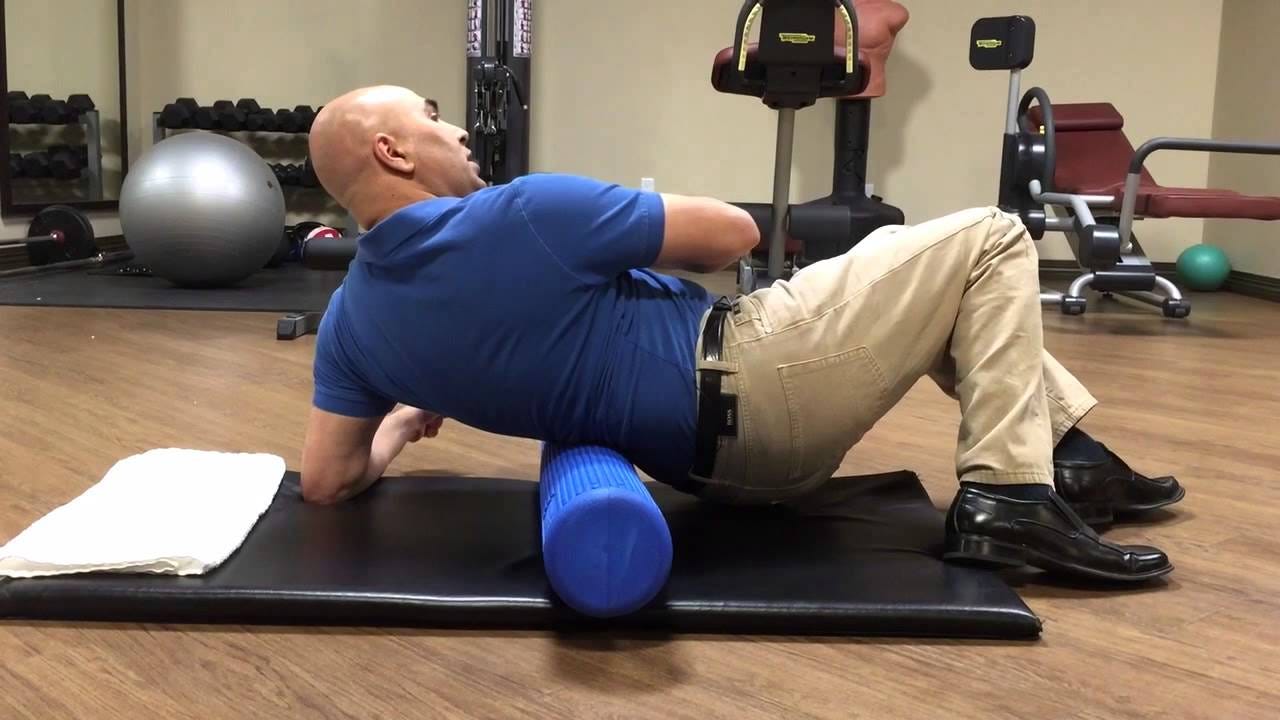
Self-myofascial release (SMR) techniques, or self-massage, would be used along Ms. F’s erector spinae and quadratus lumborum (QL) regions with the intent of reducing muscular discomfort, improving motor control, and enhancing proprioception (Shin & Sung, 2015). Figure 8.11, page 215, by Davies and Davies (2013) provides a method of SMR along the quadratus lumborum, using a small ball in a standing position to target the QL. Following SMR are corrective exercises, which are intended to: separate arm and leg movement from the lumbar spine, improve reflexive stabilization of the low back, hip, and abdominal regions, and build endurance in the aforementioned musculature. Furthermore, the exercises are designed to resist lumbar motion in the sagittal, frontal, and transverse planes. The following will explore an anti-sagittalplane exercise, known as the curl-up (not to be confused with typical sit-ups or crunches), its rationale, and progressions.

Most low back pain emanates from excessive and repetitive motions of the lumbar vertebrae (McGill, 2007). Thus, it would be logical to correct such aberrations in motor control/biomechanics, as a means of attenuating provocative motions. One such exercise includes the beginner’s curl-up (McGill, 2007). The illustration can be seen in figure 7-16, page 89 (Liebenson, 2014). Here, the client assumes a supine position with one hip flexed, and the other hip extended (helps maintain a neutral lumbar spine). Hands are placed behind the lumbar spine and the elbows are onthe floor. Following the initial set-up, the client is instructed to lift the head (coaching a packed neck) and shoulders slightly off of the floor for a total of 7-8 seconds. Such time duration isometrically stimulates stabilizing muscles of the anterior core (i.e., rectus abdominis) and builds endurance, while avoiding loss of oxygen in targeted muscles (McGill, 2007). Finally, ensuing progressions are implemented only if the current exercise is done correctly, without coaching, and is pain-free.

A progression of the beginner’s curl-up is the intermediate curl-up. All set-ups are identical to the beginner’s curl-up, with the exception of elbow position. In the intermediate curl-up, the client is encouraged to pack the neck, lift the head slightly off of the floor with the shoulders, in addition to slightly elevating the elbows off the floor (McGill, 2007). Such a position transfers more load to the rectus abdominis, compared to the beginner’s curl-up (McGill, 2007).

The advanced curl-up has the same set-up as the intermediate curl-up, with the exception of pre-bracing the abdomen. Such pre-bracing can be facilitated by an exercise professional/medical professional via fascial raking (i.e., gripping the abdominal wall with the hands to stimulate contraction). The rationale is to provide another means (i.e. voluntary and reflexive) to stimulate co-contraction of the core, thereby increasing stability and resisting motion of the lumbar spine in the sagittal plane. Illustration 7-12, page 98 by Liebenson (2014) demonstrates co-contraction of spinal stabilizers, and its effect on maintaining a neutral spine.
The aforementioned SMR techniques, curl-up progressions, and rationale are by no means considered exhaustive and/or complete; there are many other exercises and progressions that have been omitted (i.e., regressions and progressions of anti-transverse plane motions, anti-frontal plane motions, and movements to separate arm and leg motion from trunk motion). However, it is evident that rehabilitating and reinforcing the lumbar spine demands scrupulous, pragmatic, and evidence-based protocols. If one wishes to return clients back to activities of daily living with more stamina, pain-free status, and vigor, such approaches are paramount.
References
Cook, G. (2016). The Three Rs. Retrieved from http://graycook.com/?p=1553
Davies, C., & Davies, A. (2013). The trigger point therapy workbook: Your self-treatment guide for pain relief(3rded.). Oakland, CA: New Harbinger Publications.
Liebenson, C. (2014). Functional training handbook. Philadelphia, PA: Wolters Kluwer.
McGill, S. (2007). Low back disorders: Evidence-based prevention and rehabilitation(2nded.). Windsor, ON: Human Kinetics.
Page, P., Lardner, R., & Frank, C. (2010). Assessment and treatment of muscle imbalances: The Janda approach.Champaign, IL: Human Kinetics.
Shin, M. S., & Sung, Y. H. (2015). Effects of massage on muscular strength and proprioception after exercise-induced damage. Journal of Strength and Conditioning Research, 29(8), 2255-2260.
Sueki, D. G., Cleland, J. A., & Wainner, R. S. (2013). A regional interdependence model of musculoskeletal dysfunction: Research, mechanisms, and clinical implications. Journal of Manual and Manipulative Therapy, 21(2), 90-102.
-Michael McIsaac