
Body composition (BC) can be defined as the proportions of various tissues (i.e., fat, muscle, and bone) making up the body, which is generally expressed as percent body fat and percent lean body mass (Lee & Nieman, 2013). As such, knowing BC can help one track changes during weight loss or weight gain programs, in addition to determining the effectiveness of nutritional and exercise interventions. As a means of appreciating such BC measuring tools, the following will briefly consider the most frequently used BC methods, in addition to their strengths and limitations: body mass index, waist circumference, skinfold calipers, and bioelectrical impedance.

Body mass index (BMI) is one of several indices used for assessing bodyweight relative to height. The advantages of a BMI include convenience, ease of use, and a familiarity of its purpose by many within society (Lee & Nieman, 2013). BMI is still used in present day because it (height relative to weight) is considered a distinguishing feature among other markers such as age, sex, and race (Lee & Nieman, 2013). BMI is determined by dividing an individual’s weight (in kilograms) by height (in meters squared). Additionally, BMI defines overweight as ≥ 25 kg m2 and obesity as BMI ≥ 30 kg m2(He et al., 2015).Lee and Nieman (2013) also stated that BMI correlated well with other estimates of body composition such as body density, total body water, and body potassium. Essentially, such associations allowed BMI to become considered a reliable and convenient measure of obesity/adiposity. However, BMI does contain some limitations; if a person is muscular or has excessive edema (swelling), BMI will overestimate total bodyfat. Conversely, if a person has low muscle mass (i.e., elderly), BMI will underestimate total bodyfat (Lee & Nieman, 2013).
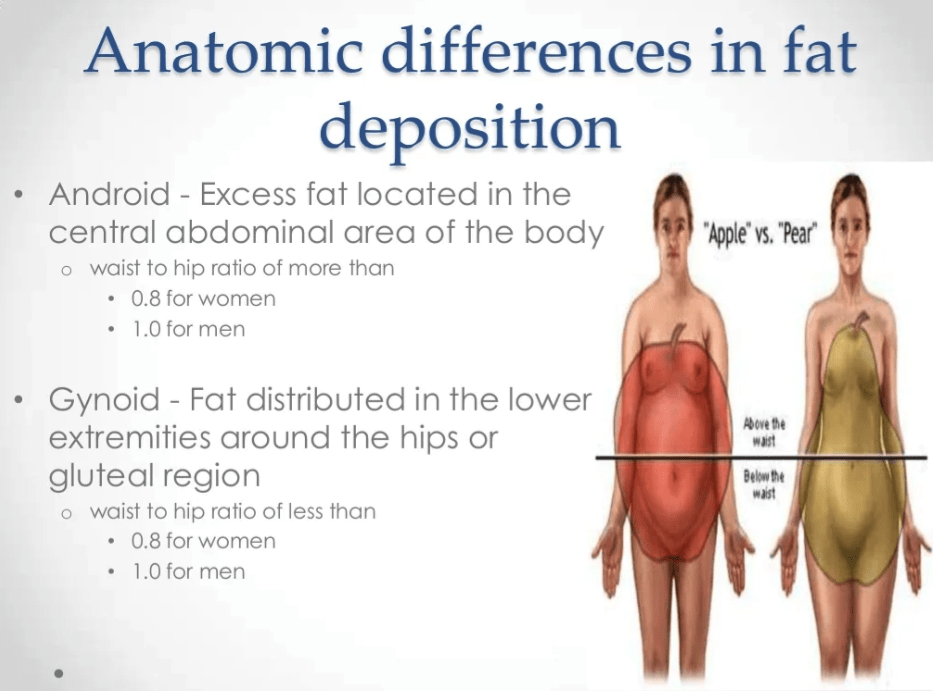
Body fat distribution is another means of gaining insight into the health status of individuals. Lee and Nieman (2013) indicated that the location fat along the body is more relevant and telling of overall health than quantity of fat. The researchers classified two main types of fat distribution: upper body (especially along the abdomen) known as android obesity, and lower body (along the hips and thighs) known as gynoid obesity (Lee & Nieman, 2013). Interestingly, the risk of insulin resistance, hyperinsulinemia, prediabetes, type 2 diabetes, hypertension, hyperlipidemia, stroke, and risk of death are increased among individuals with android obesity (Lee & Nieman, 2013). Moreover, fat along the waist is an independent risk predictor of said aberrations in health, even when BMI is normal.

Body fat distribution can be measured in several ways. However, the most convenient and cost- effective means is through waist circumference (WC). Such a measure is calculated by locating the top of the iliac crest (hip bone) while placing the measuring tape, in a level fashion, around the waist. Measurement is taken after the individual performs a normal exhale (Lee & Nieman, 2013). WC is not only simple and effective; when comparing WC to BMI, the researchers indicated that WC is a better predictor of health risks associated with obesity, over and above BMI (Lee & Nieman, 2013). As such, the waist circumference measures considered to place individuals at high risk are >40 inches in males and >35 inches in females. However, there is little predictive value from implementing WC if the individual’s BMI is >35kg/m2 or if the person is <60” in height (Lee & Nieman, 2013).

Skinfold measurement (SM) is another method to assess BC; the most widely implemented tool in assessing percent body fat (Lee & Nieman, 2013). The measurement involves selecting specific sites on the body: the chest, triceps, subscapular region, midaxillary, suprailiac, abdomen, thigh, and medial calf (Lee & Nieman, 2013). A particular advantage of SM is that thetechnique is relatively inexpensive, is widely used, and non-invasive, thereby increasing accessibility and use from the public (Selkow, Pietrosimone, & Saliba, 2011). Several assumptions are made, however, regarding selected measurement sites: the thickness of the skin/subcutaneous fat is constant, thickness of the skin is negligible, thickness of subcutaneous fat is constant between individuals, fat content of adipose tissue is constant, proportion of internal to external fat is constant, and bodyfat is normally distributed (Lee & Nieman, 2013). Of all assumptions, the compressibility of adipose tissue being constant within and between individuals is the most variable, and is therefore, considered a significant source of error from SM (Lee & Nieman, 2013).
Bioelectrical impedance (BI) is the fourth method of estimating BC. The mechanism of determining percent body fat is derived from the tendency of an electrical current (when passed through the body) to experience resistance from non-conducting tissues; namely fat and cell membranes (Lee & Nieman, 2013). Such resistance or opposition from an electrical current is called impedance. A small current is passed through the body at 50HZ and the resistance from the body is measured through the instrument (Lee & Nieman, 2013). Often, the value of resistance is placed in a regression equation (within the instrument) which also includes the individual’s height, weight, and sex. Shortly thereafter, a percent body fat value is produced. Since BI operates through the medium of water in the body, hydration (or lack thereof) can impact the readout. If the individual is not properly hydrated, an overestimation of percent body fat can occur (Lee & Nieman, 2013). Thus, it is imperative that individuals are always properly hydrated to maintain accuracy of the measure.
In conclusion, there are several simple and non-invasive measures of BC. As evidenced from the previous sections, measurement techniques exhibit a duality, having both strengths and limitations. As such, this author prefers pooling techniques (i.e., BI, WC, BMI, and weight) with the intent of deriving a clearer impression of a client’s health and BC. Ultimately, such an approach should help unite BC measurement strengths while mitigating individual limitations.
References
He, W., Lei, Q., Yang, M., Jiao, J., Ma, X., Zhou, Y., … Zhu, S. (2015). Lower BMI cutoffs to define overweight and obesity in China. Obesity, 23(3), 684-691.
Lee, R. D., & Nieman, D. C. (2013). Nutritional assessment (6thed.). New York, NY: McGraw-Hill.
Selkow, N. M., Pietrosimone, B. G., & Saliba, S. A. (2011). Subcutaneous thigh fat assessment: A comparison of skinfold calipers and ultrasound imaging.Journal of Athletic Training. 46(1), 50-54.
-Michael McIsaac