
Osteoarthritis (OA) can be a source of pain, disability, and socioeconomic cost worldwide (Glyn-Jones et al. 2015). OA is also the most common joint disease globally, and affects approximately 10% of males and 18% of females over 60 years of age. Furthermore, the epidemiology of the disorder is complex and multifactorial, with genetic, biological, and biomechanical drivers (Glyn-Jones et al. 2015). As a means of appreciating OA, the following will consider its etiology, symptoms, and methods of treatment via nutritional interventions.
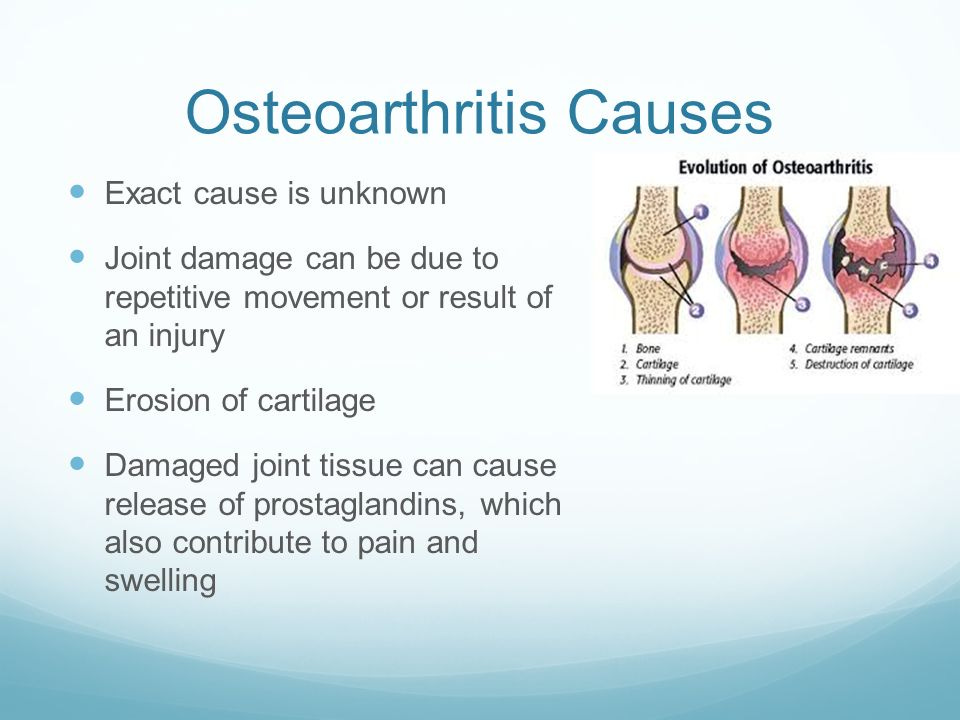
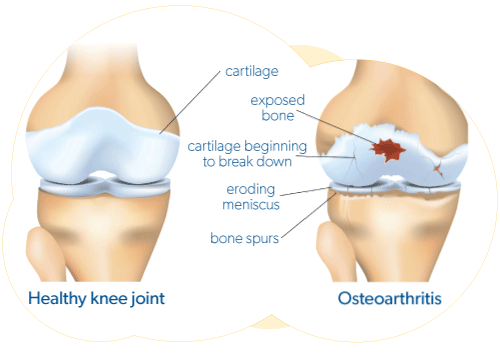
OA is an arthritic condition emanating from the degeneration of weight-bearing joints (i.e., knees and hips) (Reisner & Reisner, 2017). Generally, the disease is seen in older adults, and is considered a normal manifestation of aging. However, direct/acute trauma can also induce such changes at an earlier age. The most relevant change in OA is degeneration of the articular cartilage, which causes roughening of the articulating surfaces of the bones (Reisner & Reisner). In effect, the contacting surfaces grate against each other instead of smooth gliding actions found in a normally functioning joint.
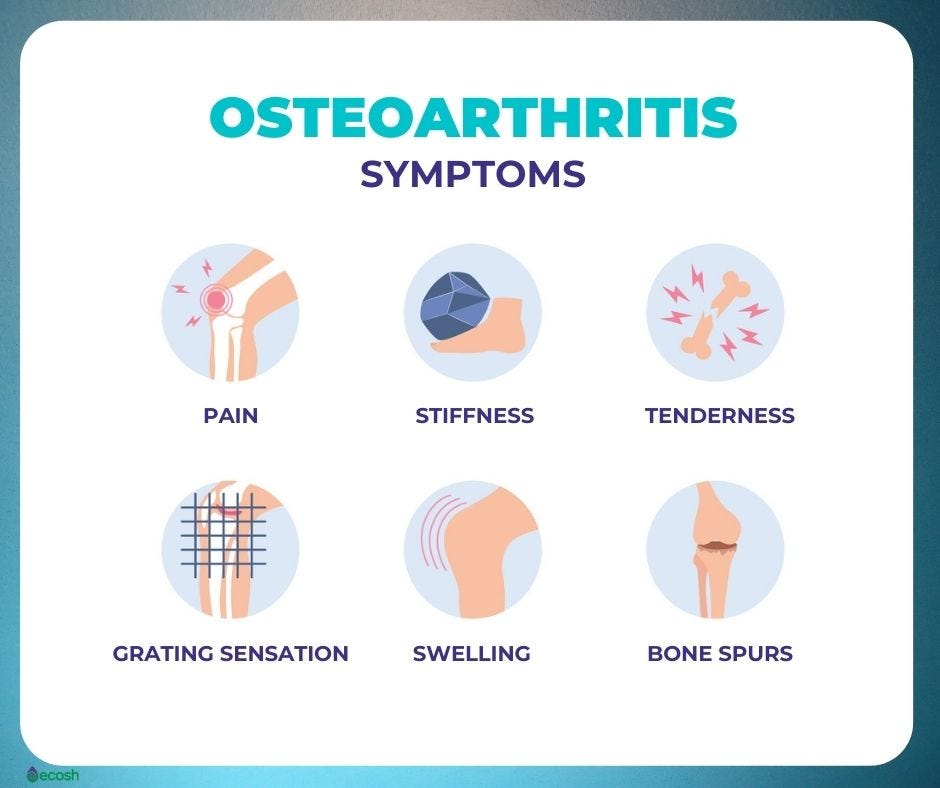
Clinical symptoms of OA include stiffness, creaking, and pain during motion of the joint. However, Reisner & Reisner (2017) noted that disability is not usually severe and the joints are not destroyed. More severe cases of OA may cause severe pain and disability, and in such cases, it is possible to replace the joint via artificial means. Such procedures are known to cause significant reductions in pain relief and improvements in joint function (Reisner & Reisner, 2017). In addition to surgery, other means do exist that can help manage pain and inflammation associated with OA. The following will consider such interventions.
Inflammation is part of joint pain and dysfunction, which is also a constituent of the chronic musculoskeletal pain cycle (CMPC) (Page, Lardner, & Frank, 2010). Inflammation is a natural immune response to clear foreign pathogens and damaged tissue, which can threaten homeostasis. However, chronic inflammation is also associated with the pain response; inflammatory mediators can induce pain by activating peripheral nociceptors (pain receptors), by promoting additional release of inflammatory mediators. Such a process sensitizes primary afferent neurons (receive and send signals to the central nervous system) to any kind of stimuli (Mironidou-Tzouvelek, 2010). One particular method of controlling the inflammatory response is through the implementation of omega-3 fatty acids (O3FAs) (Cleland & James, 2012).
Cleland and James (2012) noted that human studies on the effects of O3FAs in and its relationship to OA are lacking. However, the effects of O3FAs in-vitro (studying cell responses outside the body) and within animal models have provided mechanisms of action; such information has encouraged research in human studies (Cleland & James, 2012). For example, Cleland and James (2012) stated that eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), constituents of O3FAs, reduced the expression and release of degradative enzymes and inflammatory cytokines in an in vitro cartilage model of OA.
What is also known is that O3FAs biochemically compete with omega-6 fatty acids (O6FAs) (pro-inflammatory) in the body; both fatty acids require the same enzymes (i.e., lipoxygenase-5 and cyclooxygenase-2) when being metabolized (Ilich, Kelly, Kim, & Spicer, 2014). Thus, higher consumption of one polyunsaturated fatty acid can dominate and exert its affect upon the other, building a case for higher O3FAs consumption and controlled ingestion of O6FAs. However, it should be emphasized that further research must be done in human trials (i.e., multiple dosing levels).

In conclusion, O3FA supplementation has shown promise in controlling low-grade systemic inflammation in addition to improvements found during in-vitro and animal model research with osteoarthritic joints. Although more investigation needs to be conducted in human trials, much research has already shown that most individuals consume inadequate levels of O3FA in the diet, regardless of the presence of OA (Ilich et al., 2014). Such knowledge builds a case for additional O3FA consumption for general health, and possible benefit in managing the inflammatory affects of OA.
References
Cleland, L. G., & James, M. J. (2012). Omega‐3 fatty acids and synovitis in osteoarthritic knees. Nature Reviews Rheumatology, 8(6), 314-315.
Glyn-Jones, S., Palmer, A. J. R., Aricola, Price, A. J., Vincent, T. L., Weinans, H., & Carr, A. J (2015). Osteoarthritis. The Lancet, 386(9991), 376-387.
Ilich, J. Z., Kelly, O. J., Kim, Y., & Spicer, M. T. (2014). Low-grade chronic inflammation perpetuated by modern diet as a promoter of obesity and osteoporosis. Archives of Industrial Hygiene and Toxicology, 65(2), 139-148.
Mironidou-Tzouvelek, M. (2010). Inflammation and pain. Annals of general psychiatry, 9(1), S2-S2.
Page, P., Lardner, R., & Frank, C. (2010). Assessment and treatment of muscle imbalances: The Janda approach. Champaign, IL: Human Kinetics.
Reisner, E. G., & Reisner, H. M. (2017). An introduction to human disease: Pathology and pathophysiology correlations (10th ed.). Burlington, MA: Jones & Bartlett Learning.
-Michael McIsaac