
Pathophysiology helps us understand the pathology and physiology behind diseased and disordered systems of the body. In my last post, I covered roles of the cardiovascular system and the diseased states that occurred within it. Now, I would like to cover the pathophysiology behind these diseased states, as a precursor to anticipate, treat and prevent disease of the cardiovascular system.
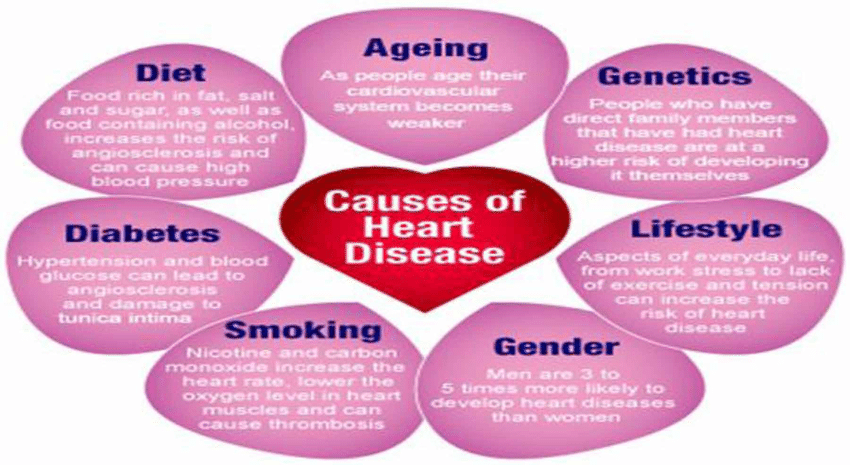
The etiology of cardiovascular heart disease (CHD) is multifactorial, and the rate at which CHD progresses is determined largely by genetics and lifestyle factors. Some of these include smoking history, diet, physical activity, and stress. CHD accounts for 51% of deaths from cardiovascular disease (Kenney, Wilmore & Costill, 2012). Moreover, Kones (2011) stated that not even 1% of the population attains ideal cardiovascular health, and one person dies every 39 seconds from CHD in the United States. How, then, does such a powerful disease propagate?
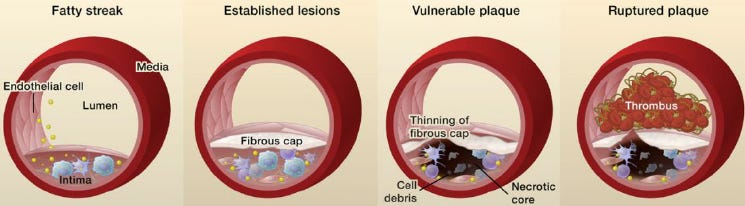
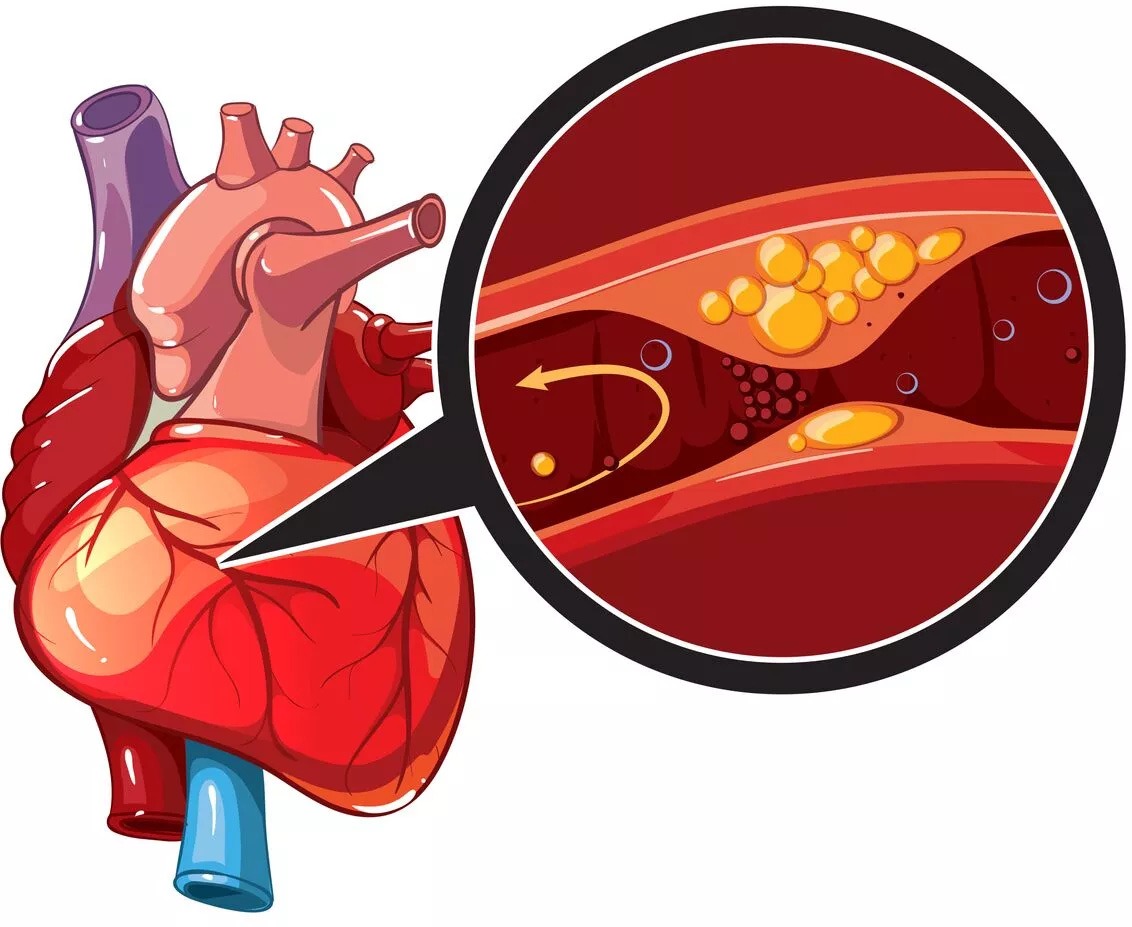
One theory posits that plaque forms as a protective mechanism to attenuate damage to the innermost lining of the artery, known as the endothelium (Kenney et al., 2012). It is hypothesized that blood platelets and monocytes migrate to the damaged endothelial layer. A substance referred to as platelet-derived growth factor is released, promoting collection of smooth muscle cells around the target tissue. Collectively, the smooth muscle cells, debris and connective tissue forms plaque (Kenney et al., 2012). Eventually, lipids settle and lock on the injury site. However, as the endothelium stabilizes, it also narrows. Colloquially, we understand this end-process as atherosclerosis.
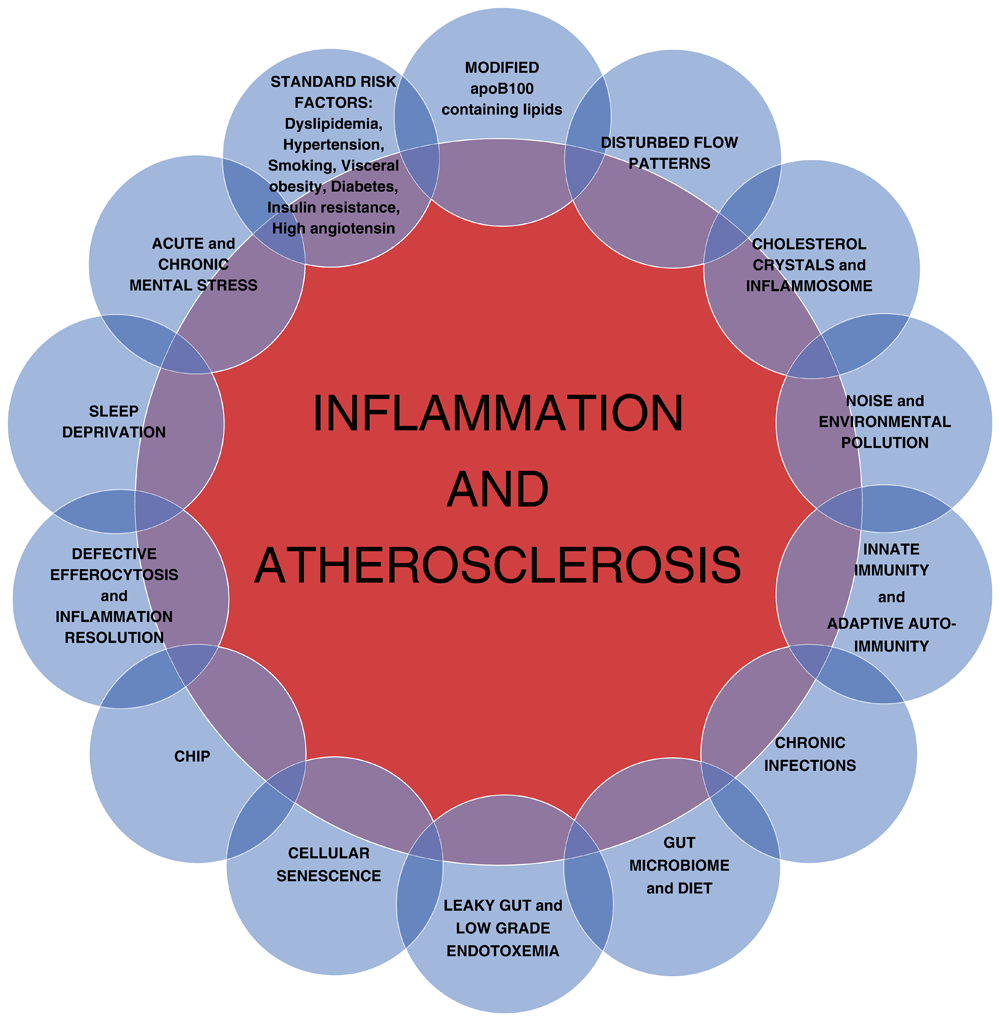
A second theory suggests that injury is not the only mechanism for arterial narrowing and plaque formation. A modification by Kenney et al. (2012) of the original theory hypothesizes that atherosclerosis is a systemic inflammatory disease. It is believed that high concentrations of cholesterol as well as free radicals from smoking, hypertension and diabetes are likely involved. Elevated homocysteine and infectious microorganisms are also considered contributing factors to arterial narrowing (Kenney et al., 2012). Of interest is in understanding the stability of plaque. Once formed, plaque contains a fibrous cap. If the plaque is thick, it tends to remain in place and stable. If it contains a thin cap, it can become unstable. This process can have serious consequences, as it encourages thrombosis, or blood clotting (Kenney et al., 2012). Free-floating clots can travel along arteries and occlude smaller arteries and arterioles. This can translate into a myocardial infarction or stroke, depending on the site of the occlusion or ischemic event.
Hypertension is another form of cardiovascular disease, constituting 7% of total leading causes of death in the United States (Kenney et al., 2012). Unfortunately, its pathophysiology is poorly understood. What we do know about the disease is that 90-95% of those people with hypertension is of unknown origin (Kenney et al., 2012). Additionally, the remaining 5-10% of people are classified as having secondary hypertension. This means that other health issues are overtaking and dominating the health status of the person, and hypertension is associated secondary to these processes.
An essential first step in treating a disease is in understanding its disordered function. Knowledge of CHD’s degenerative process allows us to become astutely aware of its beginnings. In this way, we can intervene before CHD grips the body. In this way, we can save lives.
References
Kenney, W. L., Wilmore, J. H., & Costill, D. L. (2012). Physiology of sport and exercise (5th ed.). Champaign, IL: Human Kinetics.
Kones, K., (2011). Primary prevention of coronary heart disease: Integration of new data, evolving views, revised goals, and role of rosuvastatin in management. A comprehensive survey. Drug Design, Development and Theory,5, 325–380.doi: 10.2147/DDD.S14934
-Michael McIsaac