

Excessive consumption of processed foods is a dominant trend in North America in which 70% of calories are derived from refined carbohydrates to include alcohol, vegetable oils, and sugar (Ilich, Kelly, Kim, & Spicer, 2014). Such refined sources (i.e., sugar sweetened beverages) have become linked to pathological conditions like cardiovascular disease (CVD) and insulin resistance/type 2 diabetes (Ma et al., 2016). Not only does overconsumption of refined carbohydrates contribute to said conditions, it also has been associated with retention of fluids, and sodium (Na). The following will explore the mechanisms behind such a relationship and its consequences upon cardiac function.
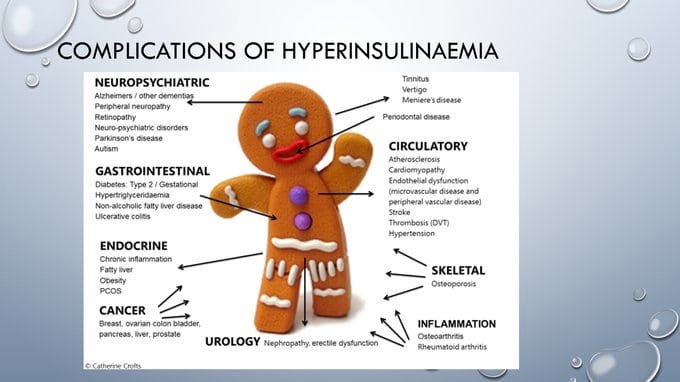
A characteristic of insulin resistance is the increased requirement of insulin (hyperinsulinemia) to store glucose and maintain serum glucose levels (i.e., <97mg/dL) (Lee & Nieman, 2013). However, hyperinsulinemia has also been associated with sodium retention, fluid retention, and hypertension (Nosadini et al., 1993). Furthermore, excessive insulin secretion has been determined as an independent risk factor for obesity, osteoarthritis, certain cancers, and Alzheimer’s disease (Crofts, Zinn, Wheldon, & Schofield, 2015). As such, chronic and excessive insulin production is associated with several physiological aberrations. The following will consider the relationship between hyperinsulinemia and Na.
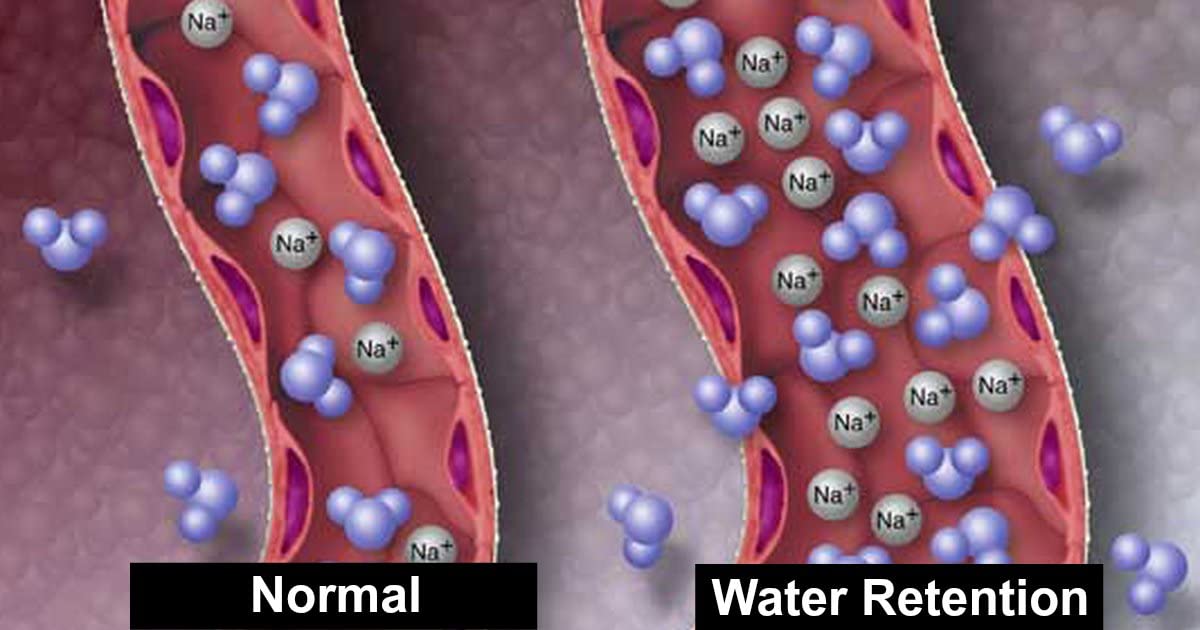
Na retention is associated with hypertension since the presence of said micronutrient in the blood increases osmotic pressure and, consequently, blood pressure (Gropper, Smith, & Carr, 2018). In type 2 diabetes (T2D), hyperinsulinemia is often secondary to impaired insulin sensitivity causing hyperglycemia and thereby escalating insulin secretion; excessive insulin production and secretion stimulates Na resorption in the proximal and distal tubule (Nosadini et al., 1993). Conversely, Nosadini et al. (1993) stated that hyperglycemia, as opposed to hyperinsulinemia, could result in a high glucose-filtered load at the renal level which could also create sodium retention and increase blood pressure (in T2D patients). Ultimately, both pathways retain Na and water thereby increasing blood pressure.
In conclusion, excessive refined carbohydrate consumption (over time) have become linked to pathological conditions to include CVD and insulin resistance/T2D (Ma et al., 2016). If cells become resistant to insulin, it might be reasonable to incorporate nutritional protocols which lower glycemic response (use of complex carbs/low carbohydrate diet, ketogenic diet) in addition to improved sleep and implementation of exercise; such approaches have been shown to control blood glucose levels and circumvent/blunt insulin secretion (Lucassen, Rother, & Cizza, 2012; Mobbs, Maistaitis, Isoda, & Poplawski, 2013; Rabol, Peterson, Dufour, Flannery, & Shulman, 2011). Ultimately, such dietary and lifestyle modifications would likely control triggers of renal absorption (i.e., hyperglycemia and hyperinsulinemia) helping lower Na/fluid retention and most relevantly, hypertension.
References
Crofts, C. A. P., Zinn, C., Wheldon, M. C., & Schofield, G. M. (2015). Hyperinsulinemia: A unifying theory of chronic disease? Diabesity, 1(4), 34-43.
Lucassen, E., A., Rother, K. I., & Cizza, G. (2012). Interacting epidemics? Sleep curtailment, insulin resistance, and obesity. Annals of the New York Academy of Sciences, 12641(1), 110-134.
Gropper, S. S., Smith, J. L., & Carr, T. P. (2018). Advanced nutrition and human metabolism (7thed.). Boston, MA: Cengage Learning.
Ilich, J. Z., Kelly, O. J., Kim, Y., & Spicer, M. T. (2014). Low-grade chronic inflammation perpetuated by modern diet as a promoter of obesity and osteoporosis. Archives of Industrial Hygiene and Toxicology, 65(2), 139-148.
Lee, R. D., & Nieman, D. C. (2013). Nutritional assessment(6thed.). New York, NY: McGraw-Hill.
Ma, J., Jacques, P. F., Meigs, J. B., Fox, C. S., Rogers, G. T., Smith, C. E., … McKeown, N. M. (2016). Sugar sweetened beverage but not diet soda consumption is positively associated with progression of insulin resistance and prediabetes. The Journal of Nutrition, 146(12), 2544-2550.
Mobbs, C. V., Maistaitis, J., Isoda, F., & Poplawski, M. (2013). Treatment of diabetes and diabetic complication with a ketogenic diet. Journal of Child Neurology, 28(8), 1009-1014.
Nosadini, R., Sambataro, M., Thomaseth, K., Pacini, G., Cipollina, M. R., Brocco, E., … Crepaldi, G. (1993). Role of hyperglycemia and insulin resistance in determining sodium retention in non-insulin-dependent diabetes. Kidney International, 44(1), 139-146.
Rabol, R., Peterson, K. F., Dufour, S., Flannery, C., & Shulman, G. I. (2011). Reversal of muscle insulin resistance with exercise reduces postprandial hepatic de novo lipogenesis in insulin resistant individuals. Proceedings of the National Academy of Sciences of the United States of America, 108(33), 13705-13709.
-Michael McIsaac