
In a previous discussion, I explored the general benefits of warm-ups and their relationships to performance enhancement. Stiff joints and restricted flexibility hinder full expressions of motions, movement patterns, and movement economy. Warm-ups can help circumvent these problems (Fradkin, Zazryn, & Smoliga, 2010). In order to more deeply appreciate the application and interventions of exercises and warm-ups, I will examine restricted ankle dorsiflexion, associated pathologies and dysfunctions, as well as evidence-based solutions to mitigate these problems.
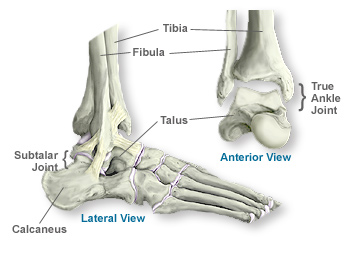
Most injuries from extracurricular activities occur within the lower extremities. 42% of these are directly related to the knee (Macrum, Bell, Boling, Lewek, & Padua, 2012). One of the mechanisms of injury is thought to be excessive motion of the patellofemoral joint in the frontal plane (Macrum et al., 2012). Macrum et al. (2012) analyzed the ankle joint to see how restricted dorsiflexion could affect leg kinematics and muscle activation patterns. Of interest was the association between patellofemoral pain and ankles; most people who have knee pain lacked dorsiflexion (Macrum et al., 2012). Additionally, Macrum et al. (2012) noted that reduced dorsiflexion caused the foot to pronate, the tibia to internally rotate, causing femoral internal rotation and valgus collapse at the knee. If these are the issues associated with restricted ankle movement, what are the solutions to restoring dorsiflexion range of motion?

Young, Nix, Wholohan, Bradhurst, and Reed (2013) performed a meta-analysis on ankle joint dorsiflexion interventions. Young et al. (2013) performed a search that included 3,362 studies. After implementing exclusion criteria, 185 studies including a total of 734 participants were reviewed (Young et al., 2013). Of the 185 studies, inclusion criteria further refined the analysis to 18 studies that were implemented in the meta-analysis (Young et al., 2013). Within the individual studies, several interventions were implemented: six studies investigated stretching with ultrasound and strengthening exercises, two studies reviewed manipulation therapy, two studies analyzed mobilization therapy, and one study investigated soleal trigger point therapy (Young et al., 2013). Results indicated that stretching alone, and in conjunction with other modalities such as ultrasound, heat, warm-ups and calf raises had statistically significant changes in ankle dorsiflexion range of motion (Young et al., 2013). The authors noted that there was insufficient evidence to support that soleal trigger point therapy, ankle joint mobilization, or manipulation yielded statistically significant gains in ankle dorsiflexion (Young et al., 2013).
Warm-ups and specific stretches not only allow for increased performance; they also assist in injury prevention and the resolution movement dysfunctions. As exemplified by the deleterious effects of stiff ankles, oversight can lead to movement impairments such as unstable knees and patellofemoral pain. Awareness and appreciation of an adequate warm-up that acknowledges performance enhancement and injury prevention, allows for a thorough, mindful, and complete program.
References
Fradkin, A., Zazryn, T.R., & Smoliga, J.M. (2010). Effects of warming-up on physical performance: A systematic review with meta-analysis. Journal of Strength and Conditioning Research, 24(1), 140-148.
Macrum, E., Bell, D.R., Boling, M., Lewek, M., & Padua, D. (2012). Effect of limiting ankle-dorsiflexion range of motion on lower extremity kinematics and muscle-activation patterns during a squat. Journal of Sport Rehabilitation. 21(2), 144-150.
Young, R., Nix, S., Wholohan, A., Bradhurst, R., & Reed, L. (2013). Interventions for increasing ankle joint dorsiflexion: a systematic review and meta-analysis. Journal of Foot & Ankle Research, 6(1), 2-18.
-Michael McIsaac