
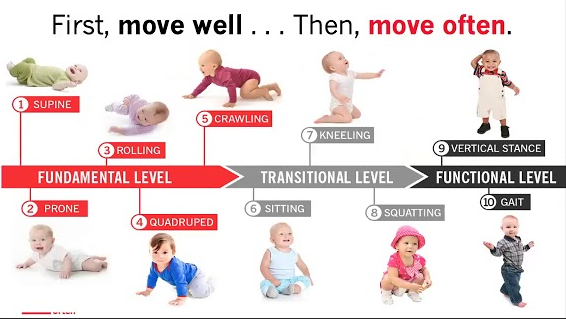
The ability to become bipedal is predicated on several developmental milestones; each reflex and motor pattern builds upon one another in a sequential and purposeful manner (Cech & Martin, 2012). In time, successful completion and mastery of the aforementioned milestones lays the groundwork for an infant to walk. One particular example of a gross motor milestone is segmental rolling. Here, the infant learns the value of rolling from supine to prone, and prone to supine leading with upper and lower body segments. Such movements teach the infant how to transition from one posture to another (Hoogenboom, Voight, Cook, & Gill, 2009). As adults, rolling patterns teach people how to rotate (i.e., throwing, shoveling, kicking, turning) in an efficient and coordinated fashion. However, segmental rolling also teaches individuals how to shift weight, cross the midline of the body, as well as coordinate movements and extremities with the core (Hoogenboom et al., 2009). As a means of appreciating, understanding, and assessing rolling patterns, the following sections will analyze a video of an individual rolling with each extremity in supine and prone positions.
- Upper Body Rolling (supine to prone leading with the left hand)
Associated YouTube link: https://www.youtube.com/watch?v=ozoI4tXOkBQ&list=PLD5Xk-dZZYNozWhprR_alt541FrozzIdO
Prior to the rolling patterns, Rodney was screened by the author for adequate left and right neck rotation, as well as left and right thoracic rotation (i.e., >30 degrees rotation) (Hoogenboom et al., 2009). Rolling pattern #1 demonstrated the participant, Rodney, implementing key motions involved in the upper body roll: left shoulder flexion/horizontal adduction leading to flexion of the trunk, following with pelvic rotation and hip flexion (Hoogenboom et al., 2009). It should be noted that Rodney is a Kinesiologist and is familiar with rolling. He was picked deliberately because he has a suspected injury to his right knee. I was interested in seeing how the injury might affect Rodney’s patterns.
The above rolling attempt was successful, in that Rodney lead the movement with his head, following with his reaching left hand across the midline. The turn was smooth with the upper body, following with his pelvis rotating after his upper body turned. Finally, Rodney’s left hip smoothly crossed midline and legs “flopped” on the floor in prone position.
- Upper Body Rolling (supine to prone leading with the right hand)
Associated YouTube link: https://www.youtube.com/watch?v=4t0j60qII-M&list=PLD5Xk-dZZYNozWhprR_alt541FrozzIdO&index=2
The above video demonstrated Rodney attempting to roll supine to prone leading with the right hand. All upper body motions happened in the proper sequential fashion according to Hoogenboom et al. (2009) in that Rodney lead with neck flexion and left rotation, followed by shoulder flexion/horizontal adduction leading to flexion of the trunk, following with pelvic rotation and hip flexion. Compared to rolling pattern #1, however, an asymmetry occurred; upon close inspection, Rodney’s right leg did not “flop” on the ground compared to the upper body roll lead by the left hand. Instead, after Rodney crossed his midline with upper body followed lower body, the right knee remained suspended for a moment, then slowly lowered to the ground. The aforementioned movement seemed suspicious as Rodney reported seeing a Physiotherapist 3 weeks ago concerning his right knee; during a soccer game, an opponent hit Rodney’s right knee, causing hyperextension and severe pain. Rodney reported awaiting an MRI to gather more information about the nature of associated pain and instability that began immediately after the accident. It should be noted that Rodney did not report pain during the rolling patterns.
- Upper Body Rolling (prone to supine leading with the left hand)
Associated YouTube link: https://www.youtube.com/watch?v=ifJLxePve9U&list=PLD5Xk-dZZYNozWhprR_alt541FrozzIdO&index=3
Rodney successfully demonstrated the upper body roll, prone to supine leading with the left hand, following the appropriate patterns outlined by Hoogenboom et al. (2009); the roll was initiated by neck extension and left rotation with left shoulder flexion and abduction of the arm crossing the midline. Trunk extension and rotation to the left occurs after arm movement, followed by left pelvic rotation and “flopping” of the left heel on the floor in the supine position.
- Upper Body Rolling (prone to supine leading with the right hand)
Associated YouTube link: https://www.youtube.com/watch?v=bKEwimF0cOs&list=PLD5Xk-dZZYNozWhprR_alt541FrozzIdO&index=4&spfreload=10
Rodney successfully demonstrated the upper body roll, prone to supine leading with the right hand, following the appropriate patterns outlined by Hoogenboom et al. (2009); the roll was initiated by neck extension and right rotation with right shoulder flexion and abduction of the arm crossing the midline. Trunk extension and rotation to the right occurred after arm movement, followed by right pelvic rotation. However, after pelvic rotation, Rodney’s right leg was “suspended” after crossing the midline; there seemed to be hesitations of letting the right leg loosely cross the body and hit the floor once in the supine position. Thus, an asymmetry existed in the aforementioned rolling pattern, when compared to rolling pattern #3.
- Lower Body Rolling (supine to prone leading with the left foot)
Associated YouTube link: https://www.youtube.com/watch?v=eYyl7u7cnCs&index=5&list=PLD5Xk-dZZYNozWhprR_alt541FrozzIdO
The lower body roll, supine to prone leading with the left foot, was successful. Rodney smoothly transitioned through all segments of the movement; the motion was initiated by flexion of the left hip, causing the leg to cross the midline, followed by right rotation of the pelvis and lumbar flexion. After lumbar flexion occurred, right rotation of the trunk followed with a “loose” upper body reaching prone position (Hoogenboom et al., 2009).
- Lower Body Rolling (supine to prone leading with the right foot)
Associated YouTube link: https://www.youtube.com/watch?v=swBKlZiuxg0&list=PLD5Xk-dZZYNozWhprR_alt541FrozzIdO&index=6
The lower body roll, supine to prone leading with the right foot, was successful, and very similar to the lower body roll, supine to prone leading with the left foot. Rodney smoothly transitioned through all segments of the movement; the motion was initiated by flexion of the right hip, causing the leg to cross the midline, followed by left rotation of the pelvis and lumbar flexion. After lumbar flexion occurred, left rotation of the trunk followed with a “loose” upper body reaching prone position (Hoogenboom et al., 2009).
- Lower Body Rolling (prone to supine leading with the left foot)
Associated YouTube link: https://www.youtube.com/watch?v=2ak7ZcBKuTE&index=7&list=PLD5Xk-dZZYNozWhprR_alt541FrozzIdO
The lower body roll, prone to supine leading with the left foot, was good overall. Rodney initiated the motion with left hip extension, causing the leg to cross the midline of the body. Following left hip extension was pelvic rotation to the left, followed by trunk extension and left rotation (Hoogenboom et al., 2009). The movement finished with the upper body “flopping” towards supine position. When comparing rolling pattern #8 found below, there was a noticeable asymmetry; one specific exception to the movement was Rodney’s non-moving (i.e., right) leg; after Rodney’s left foot loosely transitioned to the ground in supine position, his right knee seemed to stay in flexion, slowly extending after the roll was completed. This could be related to Rodney’s right knee injury.
- Lower Body Rolling (prone to supine leading with the right foot)
Associated YouTube link: https://www.youtube.com/watch?v=3Z3HFYc2Ngk&index=8&list=PLD5Xk-dZZYNozWhprR_alt541FrozzIdO
The lower body roll, prone to supine leading with the right foot, was smooth overall. Rodney initiated the motion with right hip extension, causing the leg to cross the midline of the body. Following right hip extension was pelvic rotation to the right, followed by trunk extension and right rotation (Hoogenboom et al., 2009). The movement finished with the upper body “flopping” towards supine position. Unlike Rodney’s lower body roll (i.e. #7) his non-moving (i.e., left) leg remained straight and loose as he transitioned to supine position.
In conclusion, having Rodney, an experienced Kinesiologist, perform the rolling patterns forced a deeper analysis his motor. Rolling patterns #2, #4, and #7 all exhibited some form of guarding of his right knee. If segmental rolling patterns are considered foundational movements, it would seem logical that larger, more robust, permutations (i.e., rotational movements in a bipedal position) of rolling patterns would be compromised in some fashion. Thus, analysis of segmental rolling provides an opportunity to identify and correct non-painful, dysfunctional movement patterns by an Exercise Professional. Such an approach can help facilitate smooth execution of postures and more dynamic functional tasks by enhancing the coordination of stabilizers and prime movers, all of which help reduce incidence of injury while enhancing performance (Hoogenboom et al., 2009).
References
Cech, D., & Martin, S. (2012). Functional movement development across the life span (3rd ed.). St. Louis, MO: Elsevier Health Sciences.
Hoogenboom, B.J., Voight, M.L., Cook, G., & Gill, L. (2009). Using rolling to develop neuromuscular control and coordination of the core and extremities of athletes. North American Journal of Sports Physical Therapy, 4(2), 70-82.
-Michael McIsaac