

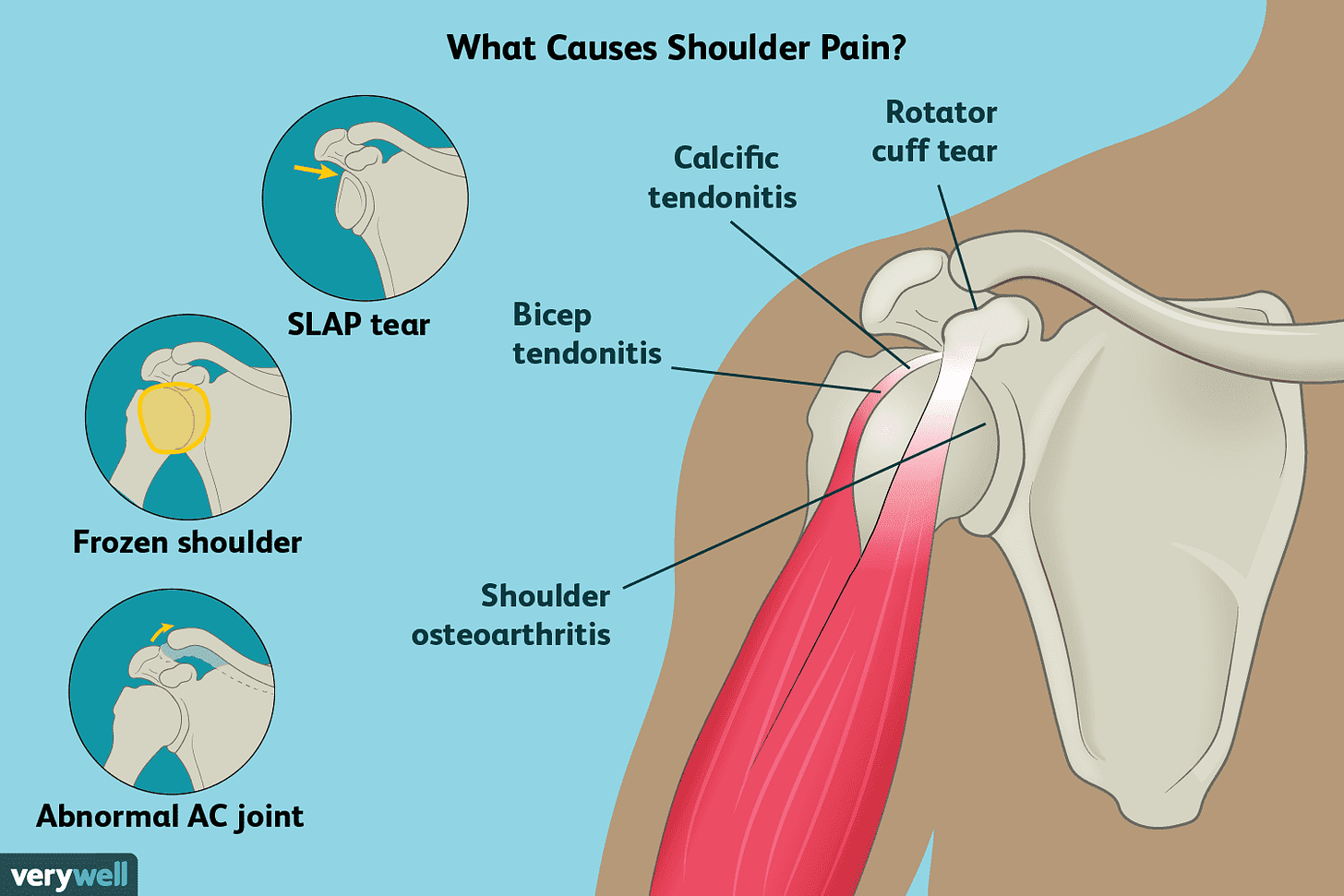
Shoulder instability is a common cause of pain within the glenohumeral (GH) joint, particularly among young athletes (Heyworth & Kocher, 2013). Although the GH joint allows a greater arc of motion compared to other joints in the body, it is also the most commonly dislocated joint in adolescents and adults (Heyworth & Kocher, 2013). Treating shoulder instability is preceded first by understanding its causes. Thus, the following will explore different permutations of GH instability as a means of understanding how to treat, and prevent, GH instability.
The GH joint is comprised of several structures, which assist in stability of the shoulder during static and dynamic motions; the capsuloligamentous and muscular structures of the shoulder serve as static and dynamic stabilizers (Heyworth & Kocher, 2013). Heyworth and Kocher (2013) noted that the dynamic stabilizers are the rotator cuff, deltoid, and scapulothoracic tendons and muscles. The aforementioned muscles and tendons work in concert exerting a compressive force on the humeral head against the concavity of the glenoid during the midrange of motion (Heyworth & Kocher, 2013). Therefore, the aforementioned interactions help centralize the head of the humerus into the center of the glenoid fossa.
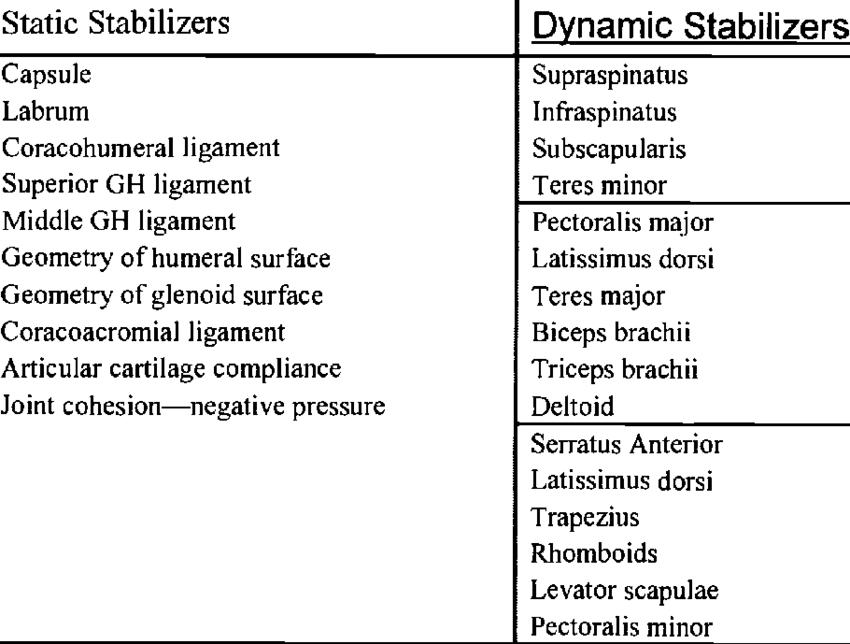
The static stabilizers are composed of the glenohumeral ligaments, capsule, labrum, and the glenoid (Heyworth & Kocher, 2013). Said structures operate at the end range of motion to limit abnormal humeral head translation. If a traumatic event compromises these dynamic and static restraints, unique patterns of disability that can limit normal shoulder function in the young athlete (Heyworth & Kocher, 2013). Thus, any injuries to static and dynamic stabilizers have the capacity to decrease stability within the GH joint.
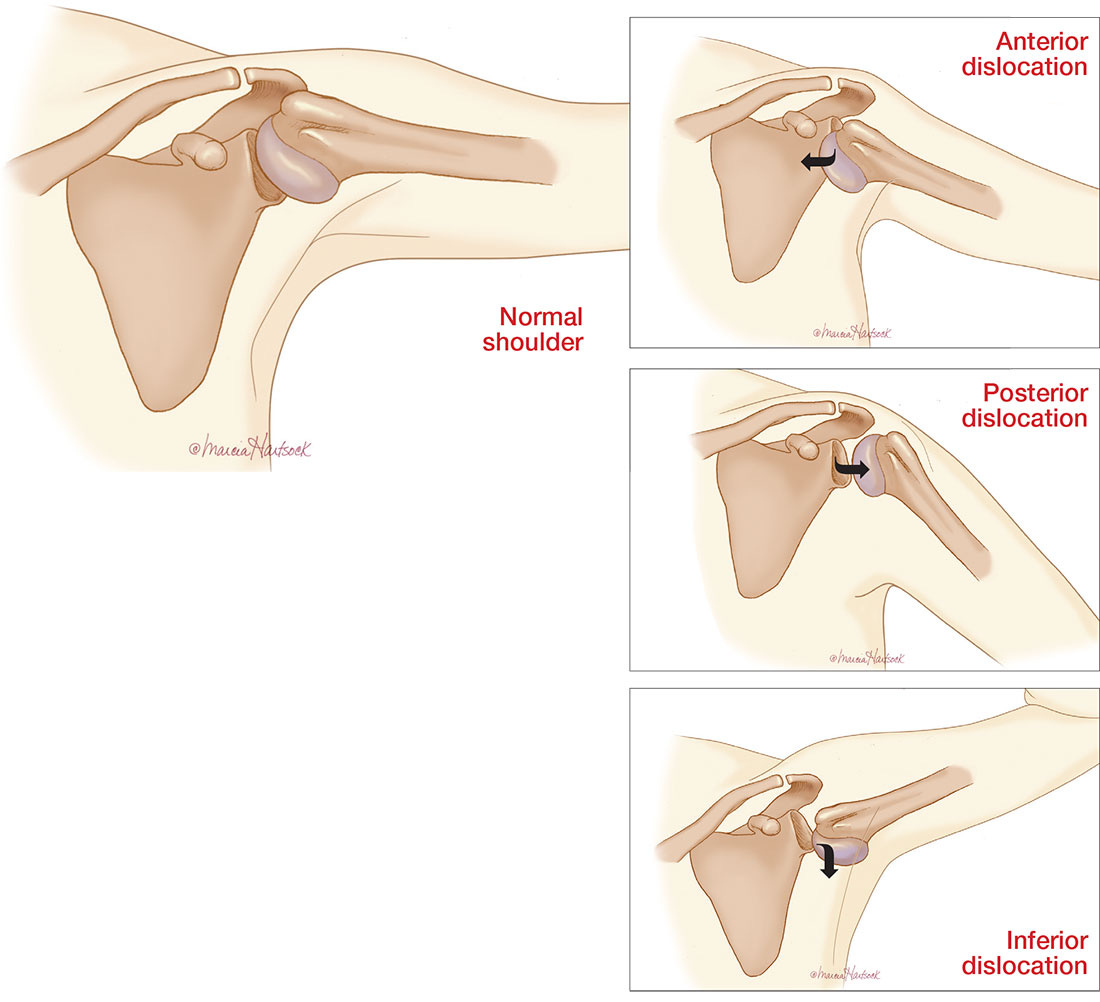
Having considered the role of static and dynamic stabilizers of the GH joint, there exist particular patterns of instability when the stabilizers are compromised. Heyworth and Kocher (2013) noted 3 specific GH joint instabilities: anterior, posterior, and multidirectional (MDI). Although there are 3 well-defined GH instability patterns, it is anterior GH instability (i.e., 85%-95% of total cases), which is the most prevalent among young athletes (Heyworth & Kocher, 2013). The origin of anterior instability is typically caused by a traumatic acute injury in contact sport. However, anterior shoulder instability can also result from a microtraumatic repetitive overuse injury typically in pitchers and throwing athletes (Heyworth and Kocher, 2013).

Having contemplated the causes and patterns of GH instability, there are solutions to restoring stability. In the capacity of exercise professionals, once cleared from a medical professional, we can assist in improving GH stability. Heyworth and Kocher (2013) stated that physical therapy should be initiated early (i.e., after 1-3 weeks of immobilization) and should focus on periscapular and rotator cuff strengthening exercises.
Heyworth and Kocher (2013) stated that after physiotherapy interventions are complete, functional, full range strengthening exercises for the scapula and GH joint are required before return to play. Exercise professionals can continue the aforementioned approaches, in addition to providing larger, more robust, exercises, which continue strengthening the rotator cuffs and scapular muscles.

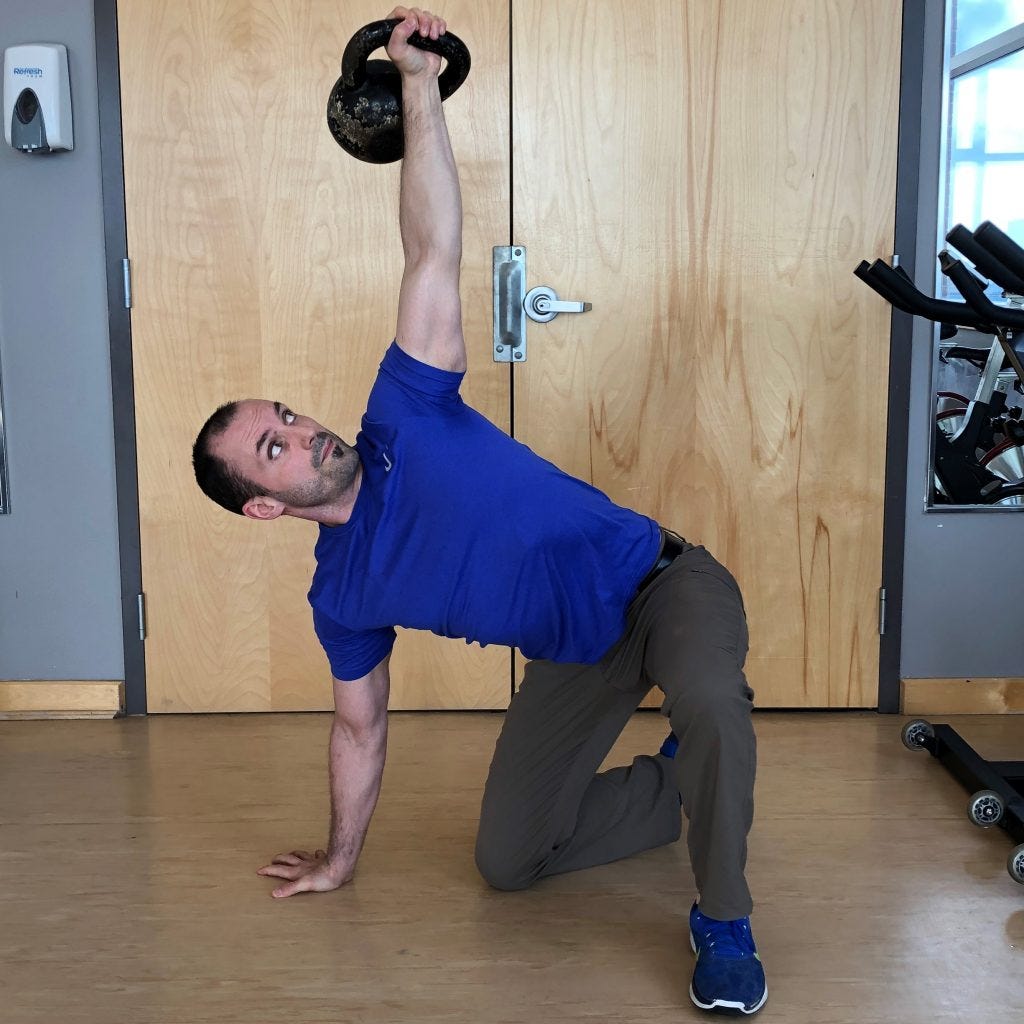
Exercises, which induce compression and distraction forces, activate muscles around the GH joint and scapula. Large, full body, exercises were recommended by Salles et al. (2015) including those, which involve the shoulder joint. Such exercises can include horizontal pushing and pulling (i.e., push-ups and seated rows, respectively) as well as vertical pushing and pulling motions (i.e., assisted chin-ups and shoulder presses/Get-Ups, respectively).
In addition to pushing and pulling motions, grip strength should also be an area of focus; evidence has supported that forceful gripping activates EMG activity of the rotator cuffs, with and without, motion at the shoulder joint. Moreover, activation of the rotator cuffs is higher during gripping motions than from inducing motion about the shoulder joint (Alizadehkhaiyat et al., 2011). Thus, it is reasonable to assume a fusion of gripping and pushing/pulling motions enhances GH joint stability and strength, based on the evidence provided.
Understanding the causes and pathomechanics of an unstable shoulder joint is paramount both in the treatment and prevention of shoulder injuries. Such knowledge enables medical/exercise professionals to develop and refine interventions specific to anterior shoulder instability by: restoring (1) pain free range of motion (2) stability of the rotator cuffs/scapular stabilizers and (3) shoulder strength (Heyworth and Kocher, 2013).
References
Alizadehkhaiyat, O., Fisher, A.C., Kemp, G.J., Vishwanathan, K., & Frostick, S.P. (2011). Shoulder muscle activation and fatigue during a controlled forceful hand grip task. Journal of Electromyography and Kinesiology, 21(3), 478-482.
Heyworth, B.E., & Kocher, M.S. (2013). Shoulder instability in the young athlete. Instructional Course Lectures, 62, 435-443.
Salles, J.I.C., Velasques, B., Cossich, V., Nicoliche, E., Ribeiro, P., Amaral, M.V., & Motta, G. (2015). Strength training and shoulder proprioception. Journal of Athletic Training, 50(3), 277-280.
-Michael McIsaac