

In the author’s practice as a Kinesiologist, the terminal goal of each client’s program is to improve the strength and quality of functional/everyday motions: pushing, pulling, squatting, lifting, carrying, and locomotion. After a client has been cleared by a medical professional to engage in exercise, a key step in the client’s post-rehabilitation (PR) program is to integrate his/her injured regions back into the aforementioned functional/everyday patterns.
To that end, the client’s program will reflect the aforementioned goals, despite what injury has occurred. What remains unique, however, is how each previously injured region is trained and reintegrated back into larger, more robust, movement patterns. The following sections will review a common shoulder dysfunction, known as shoulder impingement syndrome (SIS), as well as shoulder-strengthening protocols of Bae, Lee, Shin, Kim, and Lee (2011) and the efficacy of fusing motor control theory with strength training.
Shoulder range of motion (ROM) is unique from other joints in that articulation occurs in multiple planes (i.e., sagittal, frontal, transverse). Such a broad degree of ROM has within it, inherent instability that must be managed by the body as a means of circumventing overuse injuries and trauma (Dumont, Golijanin, & Provencher, 2014). Trauma sustained from motor vehicle accidents (MVAs) can cause tissue damage and deepen instability within the shoulder joint. Thus, soft tissue injuries of the shoulder not only impair strength; trauma can also induce aberrant motor patterns of the glenohumeral and scapulothoracic regions (Bae et al., 2011).
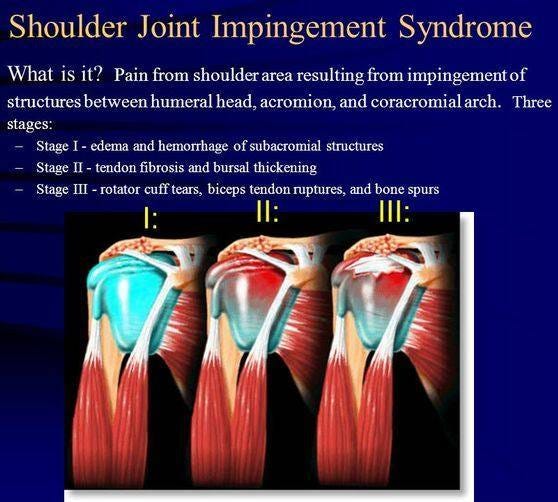
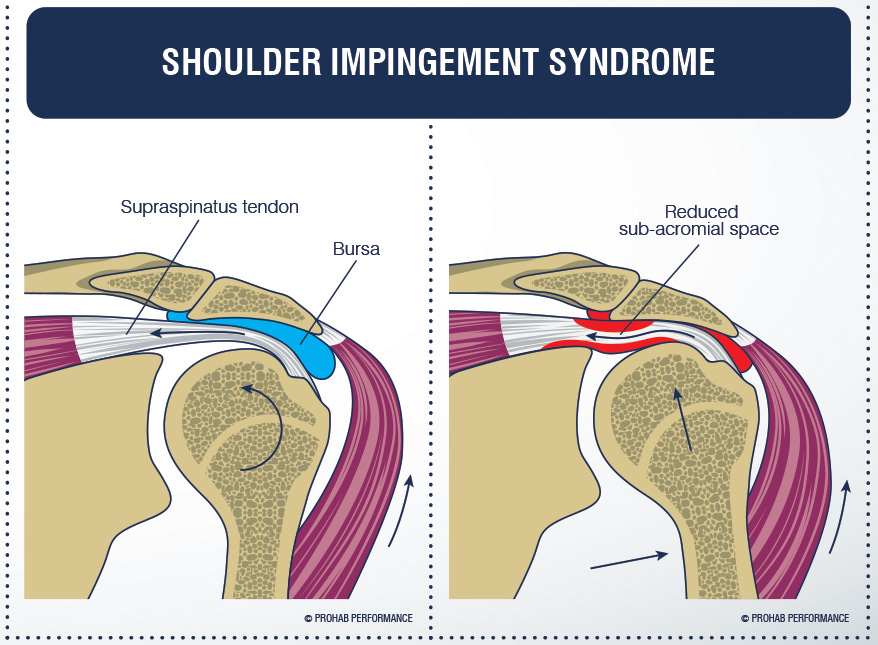
SIS is considered a disease of the shoulder, and its incidence accounts for approximately 44-65% of total shoulder diseases (Bae et al., 2011). Often, the disease presents with a prognosis of chronic pain and impairment because of restrictions in ROM. The causes of SIS can range from rotator cuff weakness, muscle imbalances, faulty movement patterns within the glenohumeral and scapulothoracic joints, as well as a poor blood supply (Bae et al., 2011).
Often, raising the arm (i.e., shoulder flexion) in the sagittal and frontal planes causes pain due to poor motor control, compromising available articulation in the subacromial space, and deepening the incidence of shoulder instability (Bae et al., 2011). Having considered the causes and characteristics of SIS, the following will review solutions to attenuating SIS.
Strength training of the shoulder joint helps the author’s clientele perform daily tasks (i.e., reaching overhead, pushing and pulling) with more ease and vigor. Although it is possible, though ill advised, to increase force output in the presence of pain and dysfunction, such an approach ignores underlying movement dysfunctions that contribute to pain. Moreover, Bae et al. (2011) provided evidence that subjects, who implemented shoulder strength training with the inclusion of a motor learning protocol, produced higher force outputs with less reports of pain than subjects who engaged in strength training as a stand-alone approach.
Bae et al. (2011) used 35 subjects who were randomly assigned to an experimental group (i.e., 17 subjects performing motor control + strengthening) and a control group (18 subjects performing strength training only). Each group participated in conservative physical therapy for 45 minutes, 3 days a week, for 4 weeks before each intervention. The experimental group underwent motor control training whereby smooth arm elevation was achieved in the sagittal, frontal, and scapular planes.
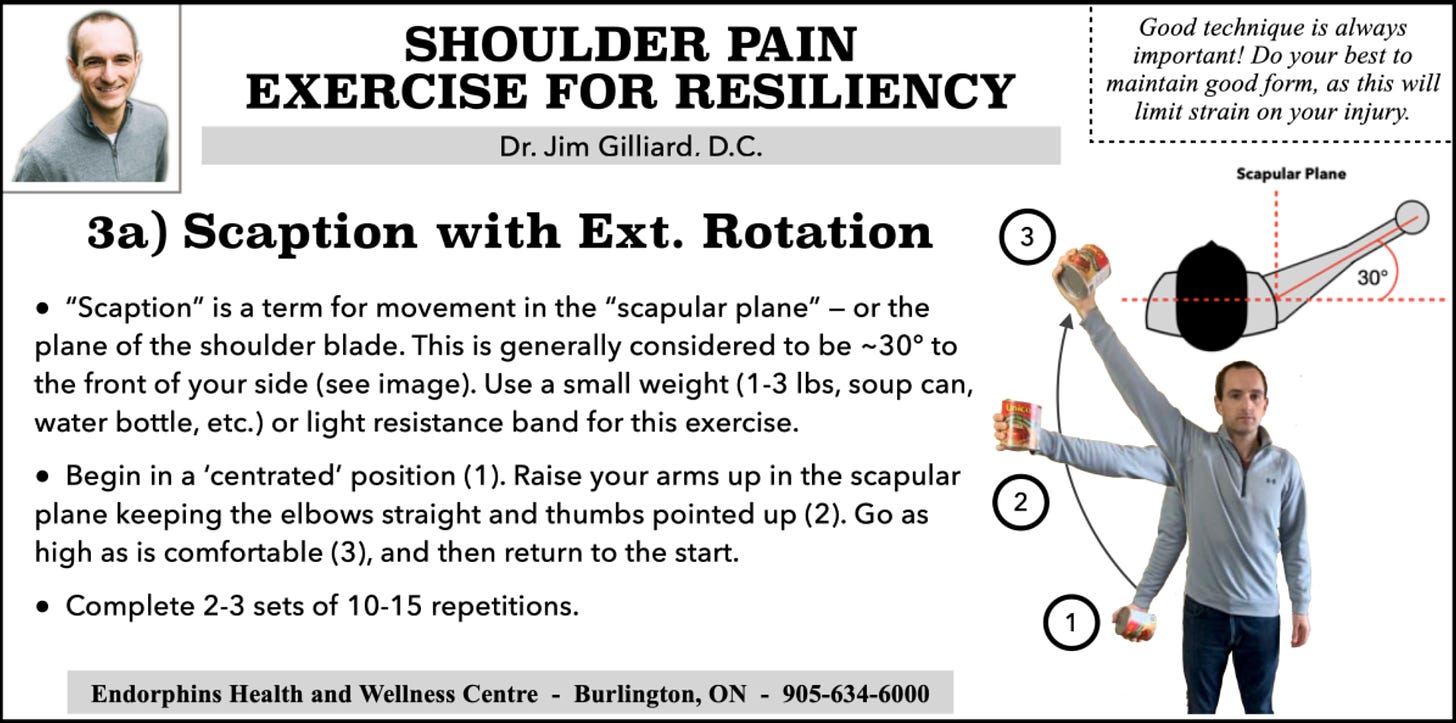
The ROM was dictated by the degree of proper motor control demonstrated by the subject; as stability was demonstrated, arm elevation increased only if pain-free ROM was reported (Bae et al., 2011). Feedback was also provided in the experimental group by physical therapists during the entire period. Once proper motor control during arm elevation was achieved, strengthening of the glenohumeral and scapulothoracic joints were achieved by: external rotation, internal rotation, scaption, chair press, push-up plus, press-up, rows, upright row (it should be noted the author does not advocate using upright rows, as they can create impingement), and exercises to engage the lower trapezius (Bae et al., 2011).

Following the 4-week intervention period, strength tests were performed in the experimental and control groups using isokinetic equipment, measuring the torque during internal rotation, external rotation at 60 degrees/sec and 180 degrees/second. Such measurements are valuable because they are considered an accurate method of measuring the motor ability of muscles (Bae et al., 2011). Normal motion at the scapulohumeral joint is predicated on properly functioning and balanced rotator cuff / scapular muscles. Normally, there exists a ratio of 2:3 for the external and internal rotator cuff muscles, and such a ratio helps maintain coupled activation of muscles and stability of the scapulohumeral joint (Bae et al., 2011).
Thus, understanding the relative strengths of the rotator cuffs is paramount in improving strength and pain-free ROM in the shoulder (Bae et al., 2011). The results between the experimental and control groups revealed compelling differences; not only did the experimental group show higher increases on several isokinetic torque measures, the experimental group also reported more favorable results on self-administered shoulder pain and disability index (SPDI) (Bae et al., 2011). Thus, motor control in combination with strength training, showed a statistically significant improvement in pain reduction, ROM, and strength increases (except for internal rotation at 60 degrees/second) compared to the control group (Bae et al., 2011).
Clients require shoulder PR that provides ample, and appropriate, nourishment to the motor control system. The aforementioned approach provides opportunities to unlearn dysfunctional movement patterns, and re-integrate appropriate movement strategies. Allowing the acquisition of motions that protect the shoulder complex enables the client to develop in a way that increases pain free and improved range of motion, function, and strength. When applied with diligence, such a method not only enhances shoulder function and force production; it also improves longevity and, ultimately, quality of life.
References
Bae, Y.H., Lee, G.C., Shin, W.S., Kim, T.H., & Lee, S.M. (2011). Effect of motor control and strengthening exercises on pain, function, strength and the range of motion of patients with shoulder impingement syndrome. Journal of Physical Therapy Science, 23(4), 687-692.
Dumont, G.D., Golijanin, P., & Provencher, M.T. (2014). Shoulder instability in the military. Clinics in Sports Medicine, 33(4), 707-714.
-Michael McIsaac