
Testosterone is an anabolic steroid synthesized from cholesterol, which is metabolized into pregnenolone and then into androstenediol or androstenedione; precursors to testosterone.1 Testosterone is responsible for maintaining function of several systems to include the immune system (lowers inflammation), neurological system (improves cognitive function), musculoskeletal system (maintains muscle mass), and aspects of the circulatory system (improves hemoglobin and hematocrit levels).1(573-574) Thus, producing and maintaining optimal testosterone levels is critical, and said steroid is heavily influenced by lifestyle and nutrition, or lack thereof. As such, the following will explore the same.
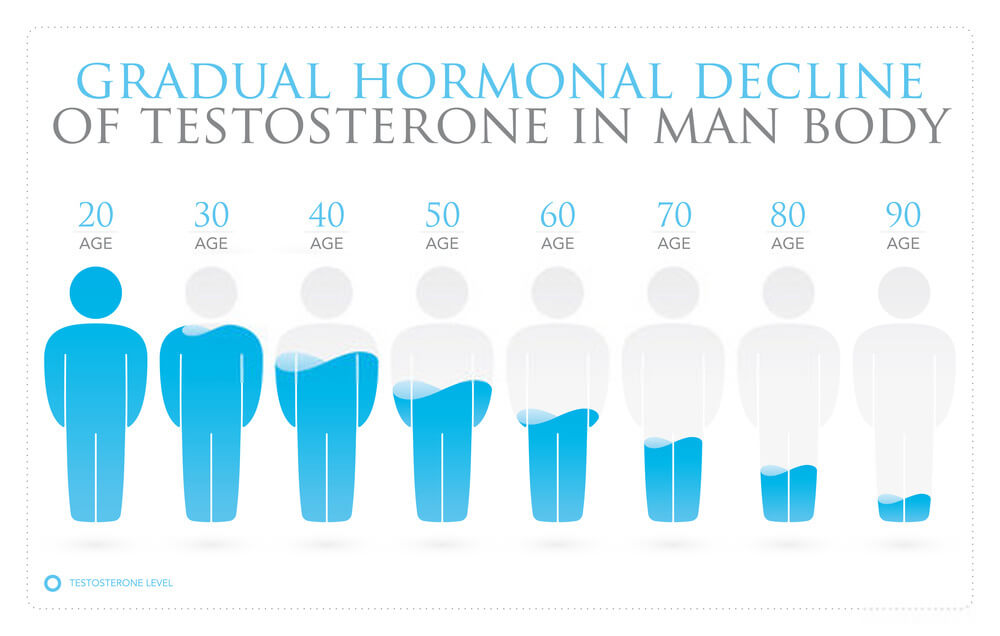
Testosterone levels in males decrease with age, obesity, and diabetes.1(573) Of the three factors mentioned, the last two are modifiable. Obesity and diabetes are closely linked to metabolic syndrome; a term that identifies an aggregate of underlying physiological aberrations intimately associated with poor health: dysregulated glucose metabolism, high blood pressure, abdominal obesity, and abnormal lipid profiles.2
If one desires to reduce risk of low testosterone, or obesity/diabetes/cardiovascular disease/stroke (ODCS), controlling said underlying risk factors is key. In particular, dysregulated glucose metabolism via insulin resistance, is thought to be the underlying and unifying pathophysiological state between ODCS.2(1)

Anton et al3 noted that on average, each American consumes over 140 lbs of added sugar per year, driving an exaggerated postprandial glucose and insulin response; such events are known to stimulate hunger levels leading to a perpetual overconsumption of added sugars and food.
Furthermore, said behaviours and habits have facilitated an obesity epidemic, defined as men who exceed 25% body fat, and women who surpass 35% body fat; measures that apply to 72% of males and 64% of females in the United States.4 Ultimately, both excessive sugar consumption and excessive adipose tissue have direct effects upon testosterone levels.
Refined sugar and refined carbohydrate intake is associated with low testosterone levels. To explore and elucidate said finding, Anton et al3(3)conducted a study from a National Health and Nutrition Examination Survey (NHANES) whereby 545 participants (males between 20-39 years of age) were included in the analysis.
Serum testosterone levels were extracted from the NHANES study amongst the subjects and compared to the amounts of sugar sweetened beverages (SSBs) consumed.3(2)Results suggested that individuals who consumed more SSBs had significant associations to lower testosterone levels, though mechanisms behind such changes were not elucidated.3(6)
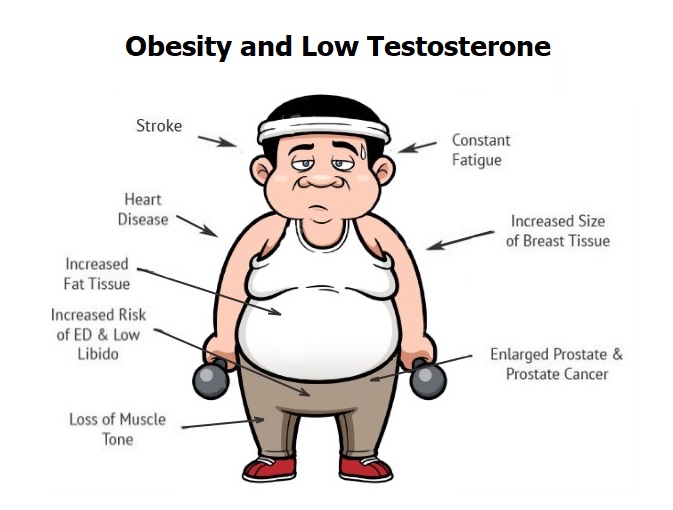
Excessive adipose tissue/obesity, conditions often caused from excessive caloric intake, also influences testosterone levels. In addition to lipid storage, adipose tissue produces steroid hormones and adipokines (cell signalling substances) to include estrogens.5 Obesity affects the production of said factors and is also associated with a chronic state of low-grade inflammation.5(90)
Of particular interest is an increased level of aromatase amongst obese individuals; the more obese individual is, the more likely low testosterone levels will be low.6Aromatase is an enzyme, which converts androstenedione (precursor to testosterone) and testosterone to estrone and estradiol, respectively.1(565)Individuals who are obese carry higher concentrations of said enzyme, especially within white adipose tissue.6(411)
In conclusion, testosterone is responsible for maintaining function of several systems to include the immune system (lowers inflammation), neurological system (improves cognitive function), musculoskeletal system (maintains muscle mass), and aspects of the circulatory system (improves hemoglobin and hematocrit levels). However, increasing rates of refined sugar consumption and obesity are closely linked to lowered testosterone levels in males. As such, it is critical that interventions are developed to lower sugar consumption and obesity amongst individuals afflicted with low testosterone levels.
References
1. Lord RS, Bralley, JA.Laboratory Evaluations for Integrative and Functional Medicine.2nd ed. Duluth, GA: Genova Diagnostics; 2012.
2. Agyemang-Yeboah F, Eghan BAJ, Annani-Akollor ME, et al. Evaluation of metabolic syndrome and its associated risk factors in Type 2 diabetes: A descriptive cross-sectional study at the komfo anokye teaching hospital, Kumasi, Ghana.Biomed Res Int. 2019. doi:https://doi.org/10.1155/2019/4562904.
3. Anton SD, Martin CK, Han H, et al. Effects of stevia, aspartame, and sucrose on food intake, satiety, and postprandial glucose and insulin levels. Appetitite. 2010;55(1):37-43. doi:10.1016/j.appet.2010.03.009.
4. Kenney WL, Wilmore, JH, Costill DL. Physiology of Sport and Exercise5th ed. Champaign, IL: Human Kinetics; 2012.5. Chen L, Xie YM, Pei JH, et al. Sugar-sweetened beverage intake and serum testosterone level in adult males 20-39 years old in the United States. Reprod Biol Endocrinol. 2018;16(61):1-7. doi:https://doi.org/10.1186/s12958-018-0378-2.
5. Zahid H, Simpson ER, Bworn KA. Inflammation, dysregulated metabolism and aromatase in obesity and breast cancer. ScienceDirect. 2016;31:90-96. doi:10.1016/j.coph.2016.11.003.
6. Seyam O, Gandhi J, Joshi G, et al. Obesity’s role in secondary male hypogonadism: A review of pathophysiology and management issues. Springer Nature Journals. 2019;1:408-418. doi:https://doi.org/10.1007/s42399-019-00056-7.
-Michael McIsaac