
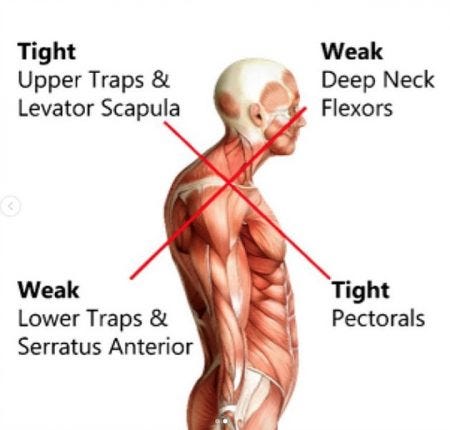
Extended periods of seated positions (i.e., desk-based work) can cause deleterious changes in posture over time. Such changes are characterized by a flexed thoracic spine, facilitated pectoralis major and minor muscles on the anterior side, in addition to facilitated upper trapezius and levator scapulae muscles on the posterior side. Conversely, the deep cervical flexors of the anterior side are inhibited, as well as the lower trapezius and serratus anterior on the posterior side (Sahrmann, 2002).
A condition known as winged scapula can arise from UCS, and this impairment becomes pronounced during flexion and extension of the arms (Sahrmann, 2002). The aforementioned dysfunctional features of the upper torso has been termed upper crossed syndrome (UCS) by a physician who, in the late 1970s, found trends in joint actions and muscle imbalances; his name was Vladmir Janda (Page, Frank & Lardner, 2014). Having considered UCS and related characteristics, the following sections will explore mitigating the effects of UCS through the application and manipulation of motor control principles, and dynamic systems theory.

Most of the author’s clientele are desk-based workers. Additionally, clientele are often recovering from motor vehicle injuries, and tend to be referred to the author for post-rehab by medical professionals and insurance companies. Clientele are generally sedentary, 40+ year old females unaccustomed to resistance training. After medical information is gathered, each client undergoes a functional movement screen.
Here, the author has an opportunity to examine the upper back and shoulder regions for unusual stiffness/restrictions and poor movement patterns/motor control. Generally, clients present with classical signs of UCS (i.e., flexed thoracic spines, anteriorly tilted shoulders, and winged scapulae).

If the thoracic spine (i.e., organismic constraint) is restricted (i.e., less that 45° left and right rotation), the author instructs the client to perform self-myofascial (SMR) release along the sides of the thoracic spine. Evidence suggests that SMR helps relax and lengthen stiff muscles (Sullivan, Silvey, Button, & Behm, 2013). When combined with stretching/mobility drills, joint range of motion (ROM) improves greater than stretching/mobility drills as stand alone modalities (Mohr, Long, and Goad, 2014).
Thus, following SMR is a thoracic mobility drill using quadruped thoracic spine rotation (UCS YouTube link below). Simple mobility drills are chosen over complex drills when possible; simpler drills are easier for the novice client to remember, as they require less joints and control thereby reducing the degrees of freedom (DOF) (Cech & Martin, 2012).
After thoracic spine mobility has been addressed, the author coaches the client through motions to “open up” or lengthen the pectoralis major and minor (i.e., organismic constraint). Again, simpler stretches and mobility drills are chosen to reduce DOF. Thus, most stretches and mobility drills occur as close to the ground as possible. One stretch that the author uses for the pectoralis major and minor muscles is the side lying pectoralis stretch (refer to UCS YouTube link below).
Side Lying Hitchhiker (Front View)
Following mobility and stretching drills for the thoracic spine and pectoralis major and minor is re-patterning of basic shoulder motions and positions. Simple external cuing is used first as a means of correcting standing shoulder positions such as “back of the head reaches the ceiling” and “sternum/chest out” (without overextending the lumbar region or elevation of the ribs). A simple exercise that further challenges maintenance of slightly retracted shoulders and a neutral thoracic spine is the farmer’s carry (refer to UCS YouTube link below).
Neutrality of the spine during said motion can be taught initially by placing a dowel (i.e., task constraint) along the spine while standing in one position. As a means of maintaining simplicity and safety, the environmental constraints are maintained (i.e., flat, non-slippery floor). After the client demonstrates competence standing with a dumbbell in each hand statically, the author encourages the client to walk in a straight line while maintaining a tall spine and slightly retracted shoulders.

The farmer’s carry can be progressed (i.e., manipulation of the task constraint) in many ways. The author uses a basic algorithm to determine progressions:
1. static/bilateral (i.e., standing still with a dumbbell in each hand)
2. dynamic/bilateral (i.e., walking a straight line with a dumbbell in each hand)
3. static/unilateral (i.e., standing still, with one dumbbell)
4. dynamic/unilateral (i.e., walking with one dumbbell)
5. static/“complex” bilateral (i.e., standing still with bottoms-up kettlebell in each hand)
6. dynamic/ “complex” bilateral (i.e., walking a straight line with bottoms-up kettlebell in each hand)
7. static/ “complex” unilateral (i.e., standing still with a bottom’s-up kettlebell in one hand)
8. dynamic/ “complex” unilateral (i.e., walking with a bottom’s up kettlebell in one hand)
In each progression listed above, the client is slowly removed from the task constraints (i.e., standing still with a dowel on the whole spine, not moving) and systematically introduced to more dynamic (i.e., static to walking) motions, and kettlebell positions that further challenge static stability (i.e., holding the kettlebell by the side to bottoms-up placement / bilateral to unilateral kettlebell placement). Mounting complexity and DOF are introduced only if the client demonstrates competency, and freedom from pain, at each level. The aforementioned examples are by no means an exhaustive representation of the author’s approach to correcting and strengthening UCS (i.e., dynamic shoulder stability in multiple planes was not introduced or explored, nor was screening of cervical ROM). However, the approach for UCS listed above does provide an opportunity to implement the principles of motor control, and dynamic systems theory in ways that are pragmatic, evidence-based, and safe.
References
Cech, D., & Martin, S. (2012). Functional movement development across the life span (3rd ed.). St. Louis, MO: Elsevier Health Sciences.
Mohr, A.R., Long, B.C., & Goad, C.L. (2014). Foam rolling and static stretching on passive hip flexion range of motion. Journal Of Sport Rehabilitation. Retrieved January 30, 2014 from http://eds.a.ebscohost.com.p.atsu.edu/eds/detail?vid=7&sid=bd6a6510-bbd3-469c-947c-
Page, P., Frank, C., & Lardner, R. (2014). The Janda approach to chronic pain syndromes: Preserving the teachings of Dr. Vladimir Janda. Retrieved January 25, 2014 from http://www.jandaapproach.com/the-janda-approach/jandas-syndromes/
Sahrmann, S. (2002). Diagnosis and treatment of movement impairment syndromes (1rst ed.). St. Louis, MO: Mosby Inc.
Sullivan, K.M., Silvey, D.B.J., Button, D.C., & Behm, D.G. (2013). Roller-massager application to the hamstrings increases sit-and-reach range of motion within five to ten seconds without performance impairments. International Journal of Sports Physical Therapy. 8(3), 228-229.
-Michael McIsaac