
![]()
In my last post, I covered a brief history of Scotland and how they circumvented vitamin D deficiencies. The intent of providing a brief history of the Scots and vitamin D intake was to show the complex interplay of environment, physiology, cultural proclivities, and economics on the effects of health. It was also my intent to contextualize the deficiency in the hopes of showing that it was possible to achieve vitamin D intake, even in the presence of apparent obstacles (i.e., poor sunlight). In this post, I would like to look more deeply into vitamin D, review a phenomenon known as Hidden Hunger, and re-evaluate the value of supplementation.
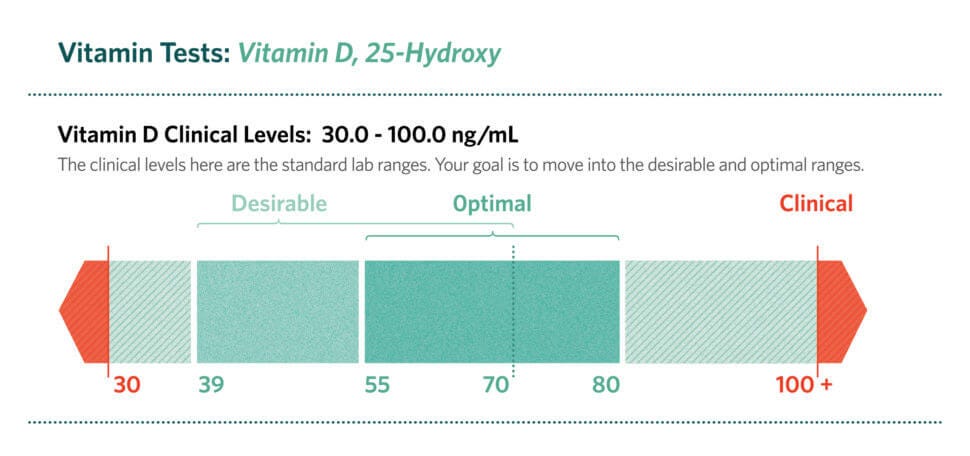
Vitamin D is comprised of a group of molecules called calciferols. The dominant forms found in the human diet are cholecalciferol (vitamin D3), ergocalciferol (vitamin D2) and 25-hydroxyvitamin D (vitamin D3, found naturally in foods) (Bendik, Friedel, Roos, Weber, & Eggersdorfer, 2014). Another unique characteristic of vitamin D3 is its ability to be synthesized through the skin by sunlight, as well as through food intake; such a characteristic helps maximize the opportunities of vitamin D absorption.
Vitamin D status is evaluated through a blood profile analyzing circulating levels of 25-hydroxyvitamin D, the summary of dietary vitamin D and vitamin D from sun exposure (Bendik et al., 2014). Once metabolized in the liver, 25-hydroxyvitamin D is converted to 1,25-dihydroxyvitamin D3, which is the active endogenous hormone responsible for many physiological actions when binding to the vitamin D receptor (VDR) (Bendik et al., 2014). If there is a redundancy mechanism (i.e., vitamin D production from sunlight and food), why do northern populations still receive inadequate levels of vitamin D (Chaplin & Jablonski, 2013)?
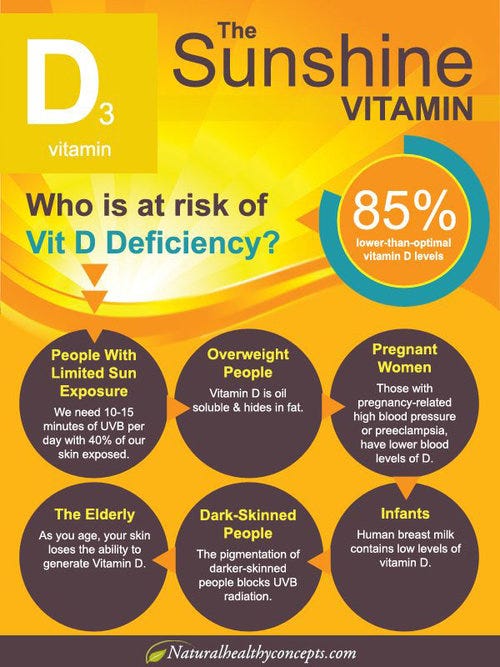
Sunlight exposure in the northern hemisphere comes from a delicate interaction of ultraviolet radiation wavelength, ozone layer thickness, solar zenith angle, geographic latitude, season of the year, and time of day (Bendik et al., 2014). Generally, the aforementioned factors limit both the quality and duration of meaningful sunlight exposure, forcing northern populations to derive most of their vitamin D through dietary means. However, due to economic and geographical limitations, many people eat adequate amounts of food, yet are still not exposed to nutrient-rich vitamin D sources (Chaplin & Jablonski, 2013). Additionally, there are no immediate signs of inadequacy, leading to the slow development of vitamin D insufficiency (Bendik et al., 2014).
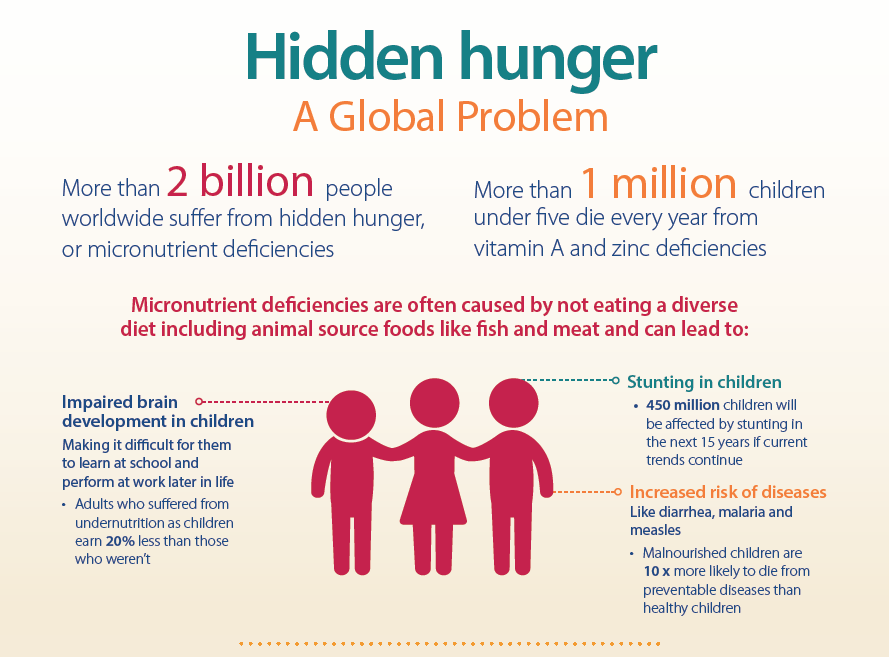
The incongruent relationship between adequate ingestion of foods, and the presence of nutrient deficiencies, is known as Hidden Hunger (Bendik et al., 2014). Interestingly, Hidden Hunger occurs in developed countries more than anticipated, and is difficult to test for initially, making the condition insidious in nature (Bendik et al., 2014). Eventually, the unfavourable amalgamation of conditions creates a potential threat to the health of a given population (Bendik et al., 2014). If Hidden Hunger exists, who are being affected?
Bendik et al., (2014) referenced a systematic review, which included 168, 389 participants worldwide spread over 200 studies, whereby serum 25-hydroxyvitamin D levels were measured. Major countries included were Europe, North America, and Asia Pacific. Other countries included the Middle East, Africa, and South America (Bendik et al., 2014). Results indicated that 6.7% of the sample was vitamin D deficient, which is also an undisputed threshold (<25nmol/L), 37.3% were vitamin D insufficient according to the International Osteoporosis Foundation (<50 nmol/L = <50 ng/mL) and 88.1% were vitamin D insufficient according to the Endocrine Society (<75 nmol/L = <30 ng/mL) (Bendik et al., 2014). If there are such widespread deficiencies and insufficiencies, is it practical to make the population eat more foods dense in vitamin D (i.e., fatty fish)?
It would seem that, although food would be an ideal method of ascertaining vitamin D, it might not be an easy protocol to implement from a public health perspective. Supplementation, however, is cheaper and although not as nutrient dense as whole foods, it does help mitigate vitamin D deficiency/insufficiency and debilitating disease (i.e. rickets) (Bendik et al., 2014). In conclusion, it is imperative to reconcile the balance between that which is ideal (i.e., natural foods dense in vitamin D) and that which is practical (i.e., supplementation), as a means of avoiding an overly pedantic approach to disease management, and embracing a method that places value on solving immediate and critical health problems.
References
Bendik, I., Friedel, A., Roos, F., F., Weber, P., & Eggersdorfer, M. (2014). Vitamin D: A critical nutrient and essential micronutrient for human health. Frontiers in Physiology, 5, 1-14.
Chaplin, G., & Jablonski, N. G. (2013). The human environment and the vitamin D compromise; Scotland as a case study in human biocultural adaptation and disease in susceptibility. Human Biology, 85(4), 529-552.
-Michael McIsaac