
Insulin resistance (IR) is an early marker, and important factor, in the development and progression of type 2 diabetes mellitus (T2D).1 Furthermore, and most relevantly, IR is likely to be present years preceding the manifestation of alterations in glycemic levels/control (i.e., hyperglycemia).1(100) As such, tracking and monitoring said biomarker could serve as a means of proactively treating and managing insulin resistance before it progresses into a deeper pathgenic state. As a means of monitoring and appreciating IR, the following will consider the same in greater detail.
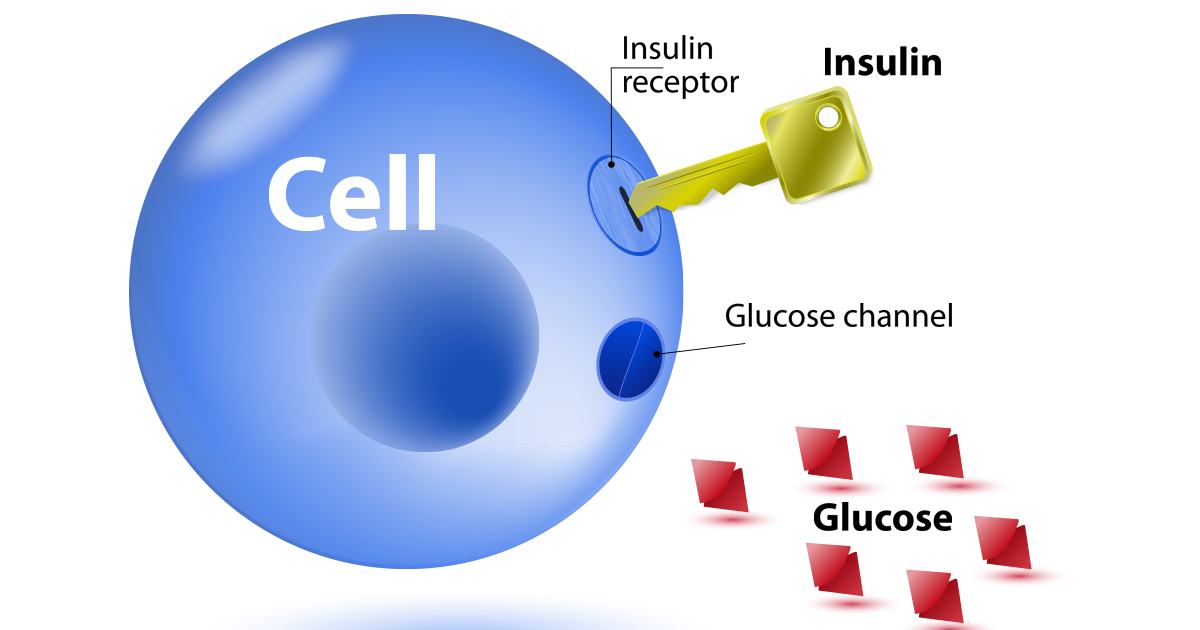
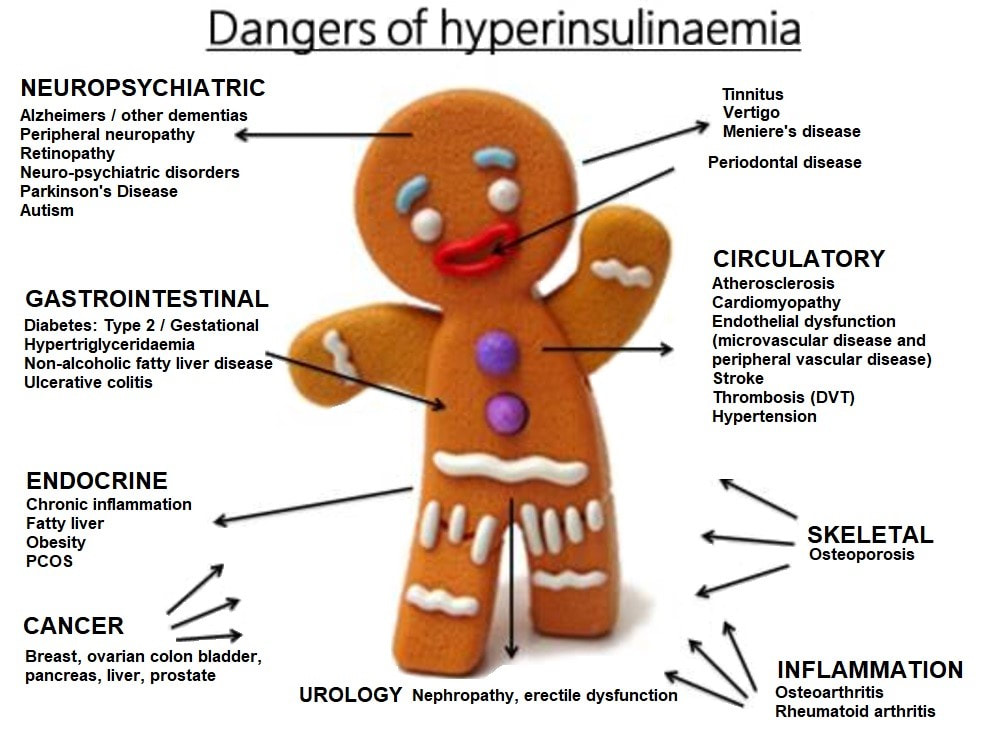
IR is a condition affecting in excess of 50 million individuals, characterized by high/normal levels of insulin present in the blood required to move glucose into cells; a condition known as hyperinsulinemia.2,3 Left unchecked, IR will not only manifest into T2D; hyperinsulinemia will also induce pathological changes in small blood vessels, nerves, contribute to atherosclerosis, as well as inhibiting the metabolism of fats and carbohydrates.4 Ultimately, hyperinsulinemia will slowly degrade organ systems in the body, eventually and inexorably contributing to aberrations in health and the development of disease states.

IR is heavily influenced by consumption of excessive quantities of refined sugars; a dietary pattern characterizing North Americans who consume in excess of 140 pounds worth per annum.5 Not only does said population consume large portions of sugar per year, North Americans also consume approximately 70% of total daily calories from refined sources to include not only sugar but vegetable oils, and alcohol.6 Such nutritional habits induce a large postprandial glucose and insulin response, which drives deeper hunger and a cyclical overconsumption of processed foods and added sugars.5(38)
Although modifying such nutritional habits are key, it is equally relevant to know if, and to what degree, IR and hyperinsulinemia are manifesting. As mentioned in the introduction, fasting glucose levels, to include hemoglobin A1C (a measure of average glucose levels over 3 months), can be at normal levels, defined as <99 mg/dL and <5.6% respectively.7 However, insulin may be compensating (hyperinsulinemia), unnoticed, in the background to maintain the aforementioned biomarkers; a metric that may screen and identify early onset of IR. Having considered the potential value and utility of monitoring and tracking insulin, the following will consider the same in greater detail.
Fasting insulin levels are considered normal if serum concentrations are below 10 IU/ml.3(556) Conversely, if fasting insulin levels are above 10 IU/ml, and glucose levels are normal (<99 mg/dL), hyperinsulinemia is likely present.3(556) Such a diagnosis can be further supported if plasma triglycerides and free fatty acids (FFAs) are also high; other hallmarks of IR/hyperinsulinemia.3(556) Ultimately, such a test, especially when combined with plasma triglyceride and FFA tests, can provide an early warning of pathogenic changes in individuals’ health before they progress into more serious forms (i.e., hyperglycemia/T2D).
In conclusion, IR is an early marker, and important factor, in the development and progression of type T2D. Furthermore, and most relevantly, IR is likely to be present years preceding the manifestation of alterations in glycemic levels and control (i.e., hyperglycemia). However, implementation and tracking of fasting insulin/plasma triglycerides/FFAs provides a fertile opportunity to modify nutrition and lifestyle habits before more serious health issues ensue.
{kind=link}
1. Cobb J, Gall W, Adam KP, et al. A novel fasting blood test for insulin resistance and prediabetes. J Diabetes Sci Technol. 2013;7(1):100-110. doi:10.1177/193229681300700112.
2. Hammaker BG. More than a coincidence: Could Alzheimer’s disease actually be a type
3 diabetes? J Diabetes Sci Technol. 28(9);2014:16-18. http://resolver.ebscohost.com.libproxy.bridgeport.edu/openurl?sid=EBSCO%3ac8h&genre=article&issn=10500758&ISBN=&volume=28&issue=9&date=20141101&spage=16&pages=16-18&title=Access&atitle=More+than+a+Coincidence%3a+Could+Alzheimer’s+Disease+Actually+Be+Type+3+Diabetes%3f&aulast=Hammaker%2c+Barbara+G.&id=DOI%3a&site=ftf-live. Accessed May 13, 2020.
3. Lord RS, Bralley, JA. Laboratory Evaluations for Integrative and Functional Medicine. 2nd ed. Duluth, GA: Genova Diagnostics; 2012.
4. Lee RD, Nieman, DC. Nutritional assessment. 6th ed. New York, NY: McGraw-Hill. 2013.
5. Anton SD, Martin CK, Han H, et al. Effects of stevia, aspartame, and sucrose on food intake, satiety, and postprandial glucose and insulin levels. Appetite. 2010;55(1):37-43. doi:10.1016/j.appet.2010.03.009.
6. Ilich JZ, Kelly, OJ, Kim Y, et al. Low-grade chronic inflammation perpetuated by modern diet as a promoter of obesity and osteoporosis. Arh Hig Rada Toksikol. 2014;65(2),139-148. doi: 10.2478/10004-1254-65-2014-2541.
7. Merino J, Leong A, Liu CT, et al. Metabolomics insights into early type 2 diabetes pathogenesis and detection in individuals with normal fasting glucose. Diabetologia. 2018;61(6):1315-1324. doi:10.1007/s00125-018-4599-x.
-Michael McIsaac